A citizen in Harare, Zimbabwe, looks at raw sewage that experts say is causing cholera, Nov. 13, 2024
Harare, Zimbabwe —
Zimbabwe has recorded new cases of cholera several months after declaring the end of an outbreak that killed more than 700 people over an 18-month period.
On Wednesday, Zimbabwe confirmed a new outbreak of cholera has been recorded in the district of Kariba — on the border with Zambia — where 21 cases have been confirmed and one person died.
Dr. Godfrey Muza, the Kariba district medical officer, said the government is working to contain the situation:
“We have set up cholera equipment camp and also some oral rehydration points within the affected villages,” said Muza. “We are getting assistance from our local and regional partners like MSF [Medecins Sans Frontieres, also known as Doctors Without Borders] and UNICEF. And our teams are on the ground doing risk communication and community engagement activities on health promotion, hygiene promotion and assisting the community in terms of improving sanction.”
In August, the Zimbabwe government declared that the 18-month long cholera outbreak was over. The outbreak affected up to 35,000 people and claimed more than 700 lives.
A billboard in Harare, Zimbabwe, encourages people to get vaccinated against cholera, Nov. 13, 2024
Zimbabwe has dealt with cholera outbreaks in the past.
In 2008, an outbreak resulted in more than 98,000 cases and more than 4,000 reported deaths.
Independent health experts such as Dr. Norman Matara of the Zimbabwe Association of Doctors for Human Rights said the government needs to address the conditions that enable the waterborne disease to spread.
“In public health, we often say cholera is a disease of poverty which mainly affects people with inadequate access to safe water and basic sanitation,” said Matara.
“In Zimbabwe, we have witnessed perennial cholera outbreaks in recent years and these outbreaks are being caused by a lack of safe drinking water supply and a broken-down sanitation system which leaves residents in densely populated communities surrounded by flowing sewer. This sewer will then contaminate alternative sources of water such as shower wells, streams, rivers and even boreholes resulting in people drinking or eating food contaminated with the cholera bacteria.”
He said that those conditions have been chronic over the years in Zimbabwe, contributing to the repeated outbreaks.
How does Zimbabwe get out of this cycle of recurring cholera outbreaks?
“We need to make sure that our hospitals are well-supposed with the real addressing solutions and medicines so that people can be assisted,” said Matara.
” … Also, those high-risk communities, especially in towns and urban cities, we may give them the oral cholera vaccine so that they may be protected. In the long term, the government needs to invest more in proper sanitation facilities and infrastructure as well as making sure that people are provided with clean safe water for drinking and cooking.”
Matara said he hopes the current outbreak is contained quickly and does not spread to other parts of Zimbabwe.
But with raw sewage flowing in some streets of Harare, it might be a question of time.
HARARE – The Health and Child Care ministry , with the support of the World Health Organization, and other partners has immunized over 200,000 people against cholera in the most vulnerable communities.
This campaign has reached 22 wards in eight districts: Chegutu, Chiredzi, Chitungwiza, Masvingo, Mhondoro-Ngezi, Mutare Rural, Mt Darwin, and Sanyati.
These targeted areas, have high artisanal mining activities where access to safe water and sanitation facilities is limited.
In these communities, clean water is scarce and health risks are high.
Hence, the vaccination campaign has brought great relief.
This initiative is beyond the numbers; it’s about saving lives and securing a healthier future.
“We remain vigilant in our efforts to strengthen our health systems and build resilience against future outbreaks,” said Health and Child Care cholera incident manager Dr Isaac Phiri.
Pelagia Chikoore, a 51-year-old resident of Venice Mine, Mhondoro Ngezi, emphasised the importance of the vaccine.
“l got vaccinated to prevent myself from getting cholera,” she said.
“Our area has a lot of mining activities, and sometimes water supply is a challenge. Although we now have a solar-powered borehole, I believe the vaccine is an extra layer of protection.”
While vaccination is not a silver bullet, it provides an additional layer of protection, especially in areas with limited access to clean water and sanitation.
Echoing Chikoore’s sentiments, 21-year-old Alice Mhembere from Mubaira shared her experience. “l know the vaccine protects me from cholera,” she said.
“We saw people getting sick because of cholera so I never hesitated when I got the opportunity.”
Cholera is a highly contagious disease that spreads through contaminated water and food.
By administering vaccines, the campaign helps to build immunity in populations at high risk, reducing the likelihood of disease spread and protecting communities from potential outbreaks for a period of 6-12 months.
Hence, it needs to be complemented by improvements in water supply and sanitation infrastructure to ensure communities are protected from another episode of cholera outbreak that claims innocent lives.
WHO played a crucial role in combating a cholera outbreak in Zimbabwe.
With unwavering commitment, WHO supported two rounds of targeted vaccination campaigns, providing the technical guidance and logistical support needed for success.
The vaccination campaigns were not only effective but also efficient, achieving over 90% coverage, and reaching the people who needed it most and making a significant impact on the community’s health.
The vaccination campaign was made possible through funding from the International Co-ordinating Group (ICG), GAVI, the Vaccine Alliance and WHO.
This collaborative effort brought hope and relief to many, showcasing the power of unity and expertise in the face of a health crisis.
“We are proud to have supported Zimbabwe in this crucial vaccination campaign. By reaching out to most vulnerable communities, we are not only preventing disease transmission but saving many lives,” said Dr Desta Tiruneh, WHO representative to Zimbabwe.
Zimbabwe’s latest cholera outbreak swelled to more than 20,000 suspected cases, but nurses and health leaders say the new, easy-to-use, rapid screening kits will make the fast-spreading infection easier to manage in future.
In the wake of a cholera outbreak that has ravaged both rural and urban communities, Zimbabwe health workers say new cholera rapid diagnostic tests (RDTs) are proving to be a game-changer.
The introduction of cholera RDTs in Zimbabwe is part of a global initiative spearheaded by Gavi, UNICEF, the World Health Organization and FIND, and will see over 1,2 million tests being distributed to 15 high-risk countries.
Previously overwhelmed by the demands of traditional cholera testing, health professionals across Zimbabwe say their workload has been reduced. After kits arrived in Harare in April, the use of RDTs is now in full swing across the country.
“The introduction of the RDTs has allowed us to diagnose suspected cholera cases within minutes. In the past we would wait for lab test results to determine whether a patient is negative or positive. The kits have helped in the containment of the disease,” said Anasia Mutero, a senior nurse at a rural clinic in Buhera district, the epicentre of the 2023–2024 cholera outbreak.
Stephen Sithole, another nurse in the district, echoed Mutero’s assertions.
“We can now test patients immediately and after 15 minutes the results will show if they are positive. We then take the correct action, saving time, and also life. The test kits have significantly improved health outcomes,” said Sithole.
Kits in action
A practical demonstration at Harare’s Beatrice Infectious Disease hospital showed the swiftness of the tests.
“Running a cholera rapid diagnostic test is relatively straightforward. The first thing is collecting a stool sample from the patient, which is then mixed with a buffer solution provided in the test kit. Drops from the mixture are added to the test strip and left undisturbed for about 15–20 minutes.
“During this time, the sample travels up the strip. If cholera bacteria are present, specific antibodies on the strip will react and produce a visible line, indicating a positive result. The whole process typically takes about 20–30 minutes from sample collection to result reading,” said Sister-in-Charge Priscilla Chizema during the demonstration.
Saving lives, curbing spread
“Without a shred of doubt, the kits have helped not only in saving lives, but also control of the spread of cholera, as patients can quickly get treatment once detected. Identifying possible cholera cases has significantly reduced the potential for outbreaks,” said Dr Collins Muchemwa, a physician at Harare Central hospital.
Director of Epidemiology and Disease Control and Neglected Tropical Diseases (NTD) in the Ministry of Health and Child Care Dr Isaac Phiri said the RDTs were a game-changer.
“We received 66,000 kits from the Vaccine Alliance [Gavi]. Prior to receiving the kits, nurses from districts and provincial hospitals across the country had undergone trainings. We want every nurse across the country to be trained. The kits are an important tool in the detection of cholera as we can quickly test for cholera in suspected cases and if the results are positive the patient is put under treatment,” said Dr Phiri.
Matron Shamiso Maturure echoed Dr Muchemwa’s sentiments, but emphasised that the kits’ ease of use makes them useful at the primary health level, where restricted technical skill might rule out the deployment of more sophisticated tools.
“[The kits’] simplicity allows our ability to manage patients, reducing the burden on our resources. The RDTs meaningfully improved the capacity to respond to the disease, not only at major hospitals, but also at local clinics,” she said.
CAPTION::Health workers using the new cholera rapid diagnostic tests. Credit: Elia Ntali
“We want every nurse trained”
Since early April, some 986 nurses and 44 laboratory personnel from provincial and district-level clinics have undergone training on the use of the test kits, supported by funding from partners including the Health Resilience Fund, the European Union, the UK, Ireland, Gavi and others.
Chiredzi District nurses Moses Ndaba and Evelyn Tavarwisa were among them. “It was really enlightening: the knowledge that we acquired assisted us in case management – something which we are practising at our stations. I want to believe that the trainings have helped a lot in containing the spread of cholera,” said Ndaba.
“The training we received will go a long way in addressing the cholera-related issues. It equipped me with the knowledge and skills that we are implementing today. The results are there, and we have testimonies that the RDTs have lessened the burden of waiting for days for results,” said Tavarwisa.
According to WHO, prior to the recent arrival of new-generation RDTs, testing capabilities in the country were problematically limited.
“Between the [recent] outbreak’s onset in February 2023 and 18 January 2024, only 2,090 antigen RDTs and 2,250 culture tests were conducted across 10 health centers. Following the training, the number of antigens RDT tests skyrocketed to 9,853, a staggering 371% increase. Culture tests also saw a significant rise, reaching 6,386, reflecting a 184% increase
That growth signifies a fourfold increase in testing accessibility in rural facilities, WHO went on to point out. Empowering nurses to carry out the testing has freed up the time of more specialised laboratory workers.
More than 20,000 suspected cholera cases and more than 400 confirmed deaths were recorded since the detection of the first cholera cases in Zimbabwe last year.
A government-led cholera response, with support from development partners, was rolled out with a focus to streamline response coordination at various levels.
This included prevention and treatment interventions.
In addition, the government embarked on a programme to provide safe water by drilling solar-powered boreholes in the most affected areas.
Kadoma – During an active cholera outbreak, compiling and reporting high quality data on suspected cases – such as age, sex, location, symptoms onset, laboratory test results and treatment response – is crucial. This provides decision-makers with timely and accurate information to guide the cholera response.
To enhance reporting systems and cholera surveillance in Zimbabwe, the World Health Organization supported the Ministry of Health and Child Care (MoHCC) to conduct a data harmonization workshop in Kadoma.
The workshop aimed to address data quality gaps and update the missing cholera data across all provinces, including essential information like the effective utilisation of partner-donated resources such as cholera testing kits.
The WHO Data Harmonisation guidelines, which delineate surveillance data monitoring processes, were instrumental technical resources utilised by WHO to steer the data harmonization exercise.
Previously, data reported on cholera cases had missing information on laboratory tests conducted by healthcare workers across the country.
This shortfall undermined accountability and failed to accurately reflect the dedicated efforts of healthcare staff.
“We were putting in the hard work, but the data wasn’t reflecting that,” says Janet Jonga, manager for epidemiology and disease control at MOHCC.
“Now, we can showcase the impact of our efforts and this improved data will be instrumental in securing the resources needed to respond to outbreaks swiftly and save lives.”
Mr Jonathan Yadini, district health information officer for Hwange District commended the exercise and noted, “Previously, data from Laboratory and Surveillance was being reported separately in parallel data flow streams, leading to discrepancies in the data. This harmonisation exercise has promoted collaboration to ensure that cholera data is now accurately and comprehensively tracked through the health information database, enhancing epidemic monitoring.”
The harmonisation exercise was made possible with WHO support and enhanced data collection, with the line list completion rates soared from 70% to 95%, providing a much clearer picture of cholera transmission across the country.
Updating of laboratory data offered a comprehensive view of utilized resources, promoting better allocation.
The newly introduced district-level epidemiological curves with the up-to-date data helped to pinpoint areas experiencing challenges and enabled a more targeted community response.
Funding for this activity came from the UN Central Emergency Response Fund (CERF), and the Health Resilience Fund, (HRF supported by EU, GAVI, UK and Ireland).
WHO’s efforts have been focused but not limited to providing enabling factors to ensure early detection through equipping surveillance officers with skills for and enhanced testing of suspected cholera cases through provision of testing kits.
HO is also providing funding to ensure that data collected is transmitted daily and reflected in the situational reports of the MoHCC to promote timely information dissemination and action.
Supportive supervision visits are being undertaken periodically providing on the job mentorship.
The country now has a unified database of cases and deaths by district for the first time, enabling quick identification of areas of interventions.
This has promoted data driven decisions and interventions.
“Following this support, the MOHCC SITREP now features district level analyses thereby highlighting the situation in hotspot districts for attention,” said Mr Trevor Muchabaiwa, data manager at WHO Zimbabwe.
“We do business differently.” A revived health club has transformed into a savings club, using a business model to promote sanitation, hygiene and nutrition.
GUTU, Zimbabwe – After an opening prayer, members of the Jekesa Kuface health club in Masvingo Province’s Gutu District launched into one of their signature songs with the lyrics: “Cholera, we will not tire until we defeat you.”
Then it was time for life-saving business.
“Is everyone paid up? Because we will all suffer if we don’t keep up with our payments, cholera is no joke people, it kills,” the club’s chairman, Johnson Rwodzi, said. He went through a book with a list of names, payment details and progress on construction of toilets and other sanitation and hygiene infrastructure.
Jekesa Kuface, which translates to “brighten up the face”, is more than just a community health club is one of several health clubs recently revived with the help of the Ministry of Health and Child Care, UNICEF and partners under interventions spearheaded under the United Nations United Nations Central Emergency Response Fund (CERF) in response to Zimbabwe’s cholera outbreak.
Jekesa Kuface health club
For members, Jekesa Kuface, initially formed in 2017 before faltering due to lethargy, has become more than just a health club to fight cholera.
“We do business differently. We are an empowerment forum, a way of life. We are integrating awareness with practical interventions in health and people’s general economic welfare,” said Rwodzi.
Since its revival in January, Jekesa Kuface has transformed itself into a savings club that is using sheer business acumen to ensure that apart from being a vehicle for health education, it empowers members with resources to construct hygiene infrastructure such as toilets in an area with a history of open defecation.
In addition, it is building the resilience of members to cope with food insecurity that affects the nutrition of children and ensuring people reap some money to pay for essentials such as their children’s education.
The concept is simple, yet effective.
Each member contributes US$1 each time the club meets.
The money is pooled into a savings pot and then invested in the form of loans to members and other community members at 20% interest.
The profits go towards assisting each member to build a toilet at their homestead.
CAPTION:A member of Kujeka Kuface Health Club records details of payments and activities. The health club has transformed itself into a savings club and uses a cooperative business model to respond to health challenges.
“That way, we ensure that even those who ordinarily would not afford to construct a toilet are able to because the money is available to buy cement and other items. Put simply, we are building toilets for each other,” said Rwodzi.
He explained: “A member digs their own hole, but we help them if they are elderly. They source mesh wire for the slab and buy two bags of cement. The club chips in with three bags of cement and also helps with the labour. Once we are done, we move to the next member.”
The target is for each member’s homestead to boast of a toilet by the end of the year.
Influencing community behaviour
On some days, club members conduct clean-up exercises in the village, hoping to change the attitudes of fellow community members.
At gatherings such as funerals, weddings and community meetings, they innovate with drama, song, dance and poetry performances to capture the attention of people and attract some who are still resistant to their messages, especially men.
Only two members of the club are men, a composition that highlights the challenges of convincing men to participate in activities they traditionally view as reserved for girls and women.
CAPTION:Health clubs and village health workers are driving social, and behaviour change campaigns in Gutu district in response to cholera, malnutrition and food security challenges.
Ten health clubs have been revived or newly established since the CERF intervention kicked in at the beginning of 2024.
Realising the need to quickly act to prevent disastrous loss of lives and livelihoods during underfunded humanitarian emergencies, the UN General Assembly established CERF as a global emergency response fund in 2006.
In Zimbabwe, CERF allowed UNICEF and partners to intervene in five districts in Masvingo, Manicaland, and Matabeleland South provinces to prevent malnutrition and disease outbreak through the provision of access to safe water, sanitation and hygiene.
Toilets
Apart from provision of water infrastructure, the intervention has an emphasis on social and behaviour change underpinned by the participation of affected communities to improve awareness of safe hygiene and sanitation practices – a key factor in the prevention of waterborne diseases such as cholera.
At the core is the empowerment of village health workers (VHWs) through refresher courses and other incentives and the resuscitation or establishment of community health clubs such as Jekesa Kuface to spearhead the spread of information on critical lifesaving water, sanitation and hygiene practices.
These include construction of toilets, waste management pits, water treatment and a healthy diet for both adults and children.
In Gutu’s Rwodzi village, such ideals were seen as too lofty only a few months ago in a community where many people were either too poor or lacked information to prioritise their health and that of their children.
But the revival of the health club has changed the tide.
Rejoice Moyo is one of those whose life has changed for the better. She recalls what she describes as the “ignorant days.”
Before joining the health club, the 40-year-old mother of seven hardly regarded a toilet as a priority need.
When her infant children asked to poop, she would take them to the back of a kitchen hut.
For her and other older members of the family, nearby bushes provided enough cover to defecate away from prying eyes.
“It didn’t even occur to me that what I was doing was hazardous,” she said, clad in a blue t-shirt inscribed with anti-cholera messages.
“Our club and the Village Health Worker opened my eyes. I now have a toilet at home, I have dug pits for waste disposal and I make sure my environment is always clean,” she said.
That’s not all. She no longer fears for her children getting malnourished because the health club has introduced a system where members help each with manual labour and knowledge to establish nutrition gardens that are providing both food and income, she said.
“From this meeting I am going to sell my vegetables. My husband is unemployed so I have become the breadwinner,” said Moyo.
Authorities say they are seeing some change.
“There is a great difference,” said Absolom Madzana, the Gutu district principal environmental health technician.
“Open defecation is becoming a thing of the past because Village Health Workers and health clubs have become key drivers of the construction of toilets. We had ten toilets built within two months, which is within our target of five toilets per month,” he said, adding that six community members have been trained as builders “and have been busy at work.”
The rate of people reporting to Chimombe Rural Hospital, where Madzana is based, with diarrhoeal diseases have dropped from an average of 20 cases per month to six, while cholera cases have not been reported in recent weeks following the UNICEF funded CERF intervention, said Madzana.
But that is no reason for complacency, with village health workers knocking door-to-door and addressing community meetings for awareness and surveillance.
“I have told them to always be on alert to prevent an outbreak. It takes time to stop an outbreak and it also takes a lot of resources,” he said.
“Prevention is better than cure,” added Madzana, before addressing a meeting of Jekesa Kuface Health Club.
UNICEF’s cholera response is funded by multiple donors, including the Centres for Disease Control and Prevention; the European Civil Protection and Humanitarian Aid Operations; the Health Resilience Fund, a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; the Government of Japan; the UN Central Emergency Response Fund and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from United Parcel Service Foundation.
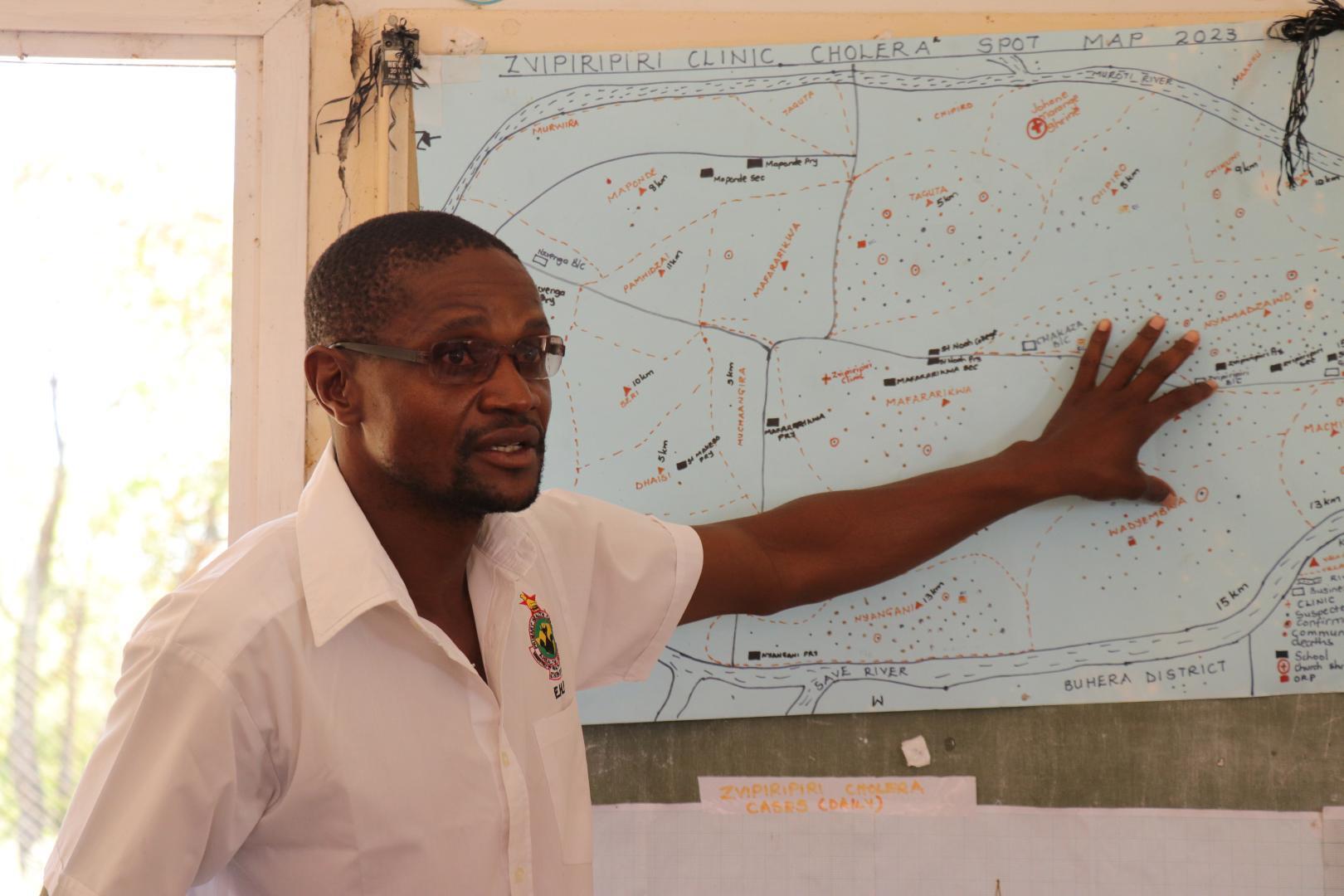
CAPTION:Zvipiripiri Rural Health Centre environmental health practitioner Lovemore Mudzingwa explaining the distribution of cholera cases
Mutare – The number of cholera cases in Zimbabwe is declining thanks to the expanded and decentralised cholera response activities undertaken by the Ministry of Health and Child Care (MoHCC), supported by WHO and other partners.
While current figures remain higher compared to the same period last year, this reduction is a welcome development, given the alarming surge between November 2023 and January this year.
At the peak of the outbreak in Manicaland province, Lovemore Mudzingwa, an environmental health practitioner (EHP) at Zvipiripiri Rural Health Centre, played a critical role.
He tirelessly responded to rumors in the community, providing essential information and disinfecting homes of suspected patients after assisting with their transportation to the clinic.
CAPTION: A CTC at Zvipiripiri
Driven by a commitment to making a difference, Lovemore works hard to ensure his community has accurate information on cholera and other diseases.
He actively identifies and addresses potential contamination sources, conducting regular inspections of water and food facilities to enforce hygiene standards.
“Our responsibility extends beyond responding to outbreaks,” says Lovemore.
“We strive to prevent them altogether. By educating communities on the importance of safe water, sanitation, and hygiene practices, we empower them to protect themselves and their families from cholera.”
Lovemore’s dedication saved lives.
In Mutorera Village, Zvipiripiri, his intervention helped 11 members of a single family survive cholera, with one succumbing to the disease.
One survivor, 21-year-old Clara Marime**, expresses her deep appreciation for Lovemore and the other health workers at Zvipiripiri.
Coming from a religious group that often avoids modern medicine, her experience was particularly challenging.
“I’m grateful to be alive,” she narrates.
“By the time I reached the clinic, I was completely disoriented. I only realized where I was a day later.”
While their efforts often go unnoticed, EHPs play a vital role in cholera outbreaks.
They manage funerals during outbreaks, coordinate emergency response efforts, and provide crucial support to affected communities.
CAPTION: A CTC at Zvipiripiri
From setting up cholera treatment centres to conducting contact tracing and disease surveillance, their expertise is vital for containing the spread of the disease and saving lives, not just from cholera.
Since February 12th, 2024, Zimbabwe has been grappling with a cholera outbreak.
As of 11 May 2024, a total of 33,914 suspected cholera cases have been reported nationwide, with 87 confirmed deaths, 623 suspected deaths, and 3,963 confirmed cases.
Manicaland province alone recorded 6,596 cases during the same period.
In Zvipiripiri, WHO leveraged funding from the Health Resilience Fund (HRF) to strengthen the cholera treatment center.
The facility was expanded from eight beds to twelve and provided essential medical supplies like rehydration fluids, antibiotics, and other cholera-specific treatment materials.
Additionally, WHO supported the installation of sanitation facilities like waste pits and emergency latrines to promote hygiene and prevent further transmission.
Triage points were also established to ensure an organized flow of patients and staff, minimizing infection risks.
Furthermore, in November 2023, WHO provided the province with essential supplies including medicines, personal protective equipment (PPE), information, education, and communication (IEC) materials, and cleaning and disinfection supplies to bolster response efforts.
In addition, WHO, with the support from HRF and Central Emergency Response Fund (UNCERF), spearheaded training programmes for EHPs, reaching over 60 individuals from all districts across the country.
These trainings focused on water quality monitoring, equipping EHPs with the knowledge and skills to effectively test and analyse water samples.
To further strengthen water quality surveillance in communities and especially in CTCs, WHO procured and distributed water quality kits and consumables.
Additionally, WHO provided training on food safety for 115 EHPs, empowering them with current food trends, standards, and knowledge on foodborne illnesses.
They gained valuable skills in preventing and controlling cholera and other diarrhoeal diseases, including vital measures to be implemented in communities and CTCs.
On the job mentorship to EHPs on infection prevention and control and community engagement activities in CTCs and communities in response to the cholera outbreak is still being provided.
“The significant decline in cholera cases in Zimbabwe is a testament to the collective efforts of the MoHCC, WHO, and other partners. However, our work is far from over. We must continue to support communities to strengthen prevention efforts to ensure a lasting impact on public health,” notes Dr Sally-Ann Ohene, WHO Zimbabwe cholera incident manager.
**Names changed to protect identity of the contributor.
Hundreds of people have died of cholera this year in Zimbabwe, where the lack of adequate water and sanitation fuels an uncontrolled outbreak.
In Zimbabwe, water supply challenges, lack of access to sanitation and hygiene, and prolonged dry seasons caused by climate change have exacerbated a cholera outbreak that has killed hundreds of people this year.
The latest outbreak began in the town of Chegutu, about 60 miles south of the capital city, Harare, where the first patient with cholera was reported in February 2023. The number of cases increased throughout 2023, spreading to 10 provinces throughout the country. Cholera cases are still rising, with 35,000 recorded cases and 600 deaths in 2024 alone.
In addition to straining Zimbabwe’s health care systems, the outbreak has exposed vulnerabilities in water, sanitation, and hygiene infrastructure in both rural and urban areas. This has heightened the risk of transmission. The limited global supply of oral cholera vaccines has further complicated response efforts. Below, two experts with Doctors Without Borders/Médecins Sans Frontières (MSF) Southern Africa explain why a new approach is needed.
By Phillip Aruna, MSF regional operations team leader, and Mounia Amrani, MSF regional medical team leader Zimbabwe is grappling with the second-largest cholera outbreak in its history, with cases rapidly spreading across the country. It started on February 12, 2023, and to date, more than 600 people have died from cholera and over 35,000 have been infected. To save lives and prevent more people from falling sick, Zimbabwe has to invest in its water sanitation and hygiene infrastructure.
Cholera is a potentially deadly disease that is caused by bacteria that live in water. Access to clean water, proper sanitation infrastructure, and hygiene measures reduce the likelihood and severity of cholera outbreaks. Recurring outbreaks in Zimbabwe are a problem caused by old and degraded water and sewage systems in urban areas. Certain cities, such as Harare, have endured months without running water, with raw sewage becoming a common sight in the densely populated suburbs.
Rural communities are affected because they are resorting to drinking unsafe water from the surrounding rivers. The lack of substantial, adequate rain has compounded the situation both in urban and rural areas, with the water table depleting.
In Zimbabwe’s Buhera District, where MSF teams supported the Ministry of Health and Child Care in the fight against cholera for three months, villagers have had to drink river water, which they shared with wild and domestic animals. Boreholes have broken down, leaving them with no other options. Unsurprisingly, cholera did not spare Buhera.
MSF also intervened in Mbire District, about 120 miles north of Harare. In Mbire, our teams noticed there was 52 percent coverage for safe water sources, while 48 percent was from the river, and a paltry 37 percent latrine coverage. When people from Mbire work their gardens and fields along the river, they consume water from the river, which is unsafe. Without toilets in the fields, community members resorted to using bush toilets along the river.
“We bathe and drink water from the stream. There is no other source of water, and we are used to this. Recently, miners started complaining of diarrhea.” — Lasten, a miner Kamudonzvo in Shamva
Mining communities are also recording a high number of cholera cases. Miners access water from contaminated sources like dumped mining pits and nearby rivers, creating a breeding ground for cholera. This is the case in Shamva district, where MSF teams recently provided support. Open defecation and limited sanitation facilities further exacerbate the situation.
Villagers have had to drink river water, which they shared with wild and domestic animals. Boreholes have broken down, leaving them with no other option. Unsurprisingly, cholera did not spare Buhera.
Another population recording a high number of cases is a conservative religious community that objects to contemporary medication. They believe in using water for bathing, which sometimes contaminates water sources. Many cases are believed to have emanated from their gatherings.
The common element between all these communities is the lack of access to clean water and adequate sewage facilities. This problem urgently needs to be addressed to control the cholera outbreaks.
In theory, cholera vaccines could also help to control the disease. Unfortunately, there’s a global shortage of oral cholera vaccines today and Zimbabwe doesn’t have enough doses to cover a wider breadth of the population.
The situation is the same anywhere else — no country has enough cholera vaccines today. This shortage is not going to be solved soon so countries shouldn’t count on vaccination to prevent or curb cholera outbreaks. This stresses the urgency of strengthening water and sanitation systems.
“We just go to the river with our containers and dig a shallow well in the sand. Once we reach the water level, we just wait for a few minutes for the unwanted particles in the water to settle down and then we fetch our water. We then destroy the shallow well by putting sand again on top of the water and we leave. This way we feel the water is safe and our elders have been doing this since time immemorial and none of them has ever complained of any stomach pains.” — Delinah, Buhera
The longer-term solutions include replacing antiquated water and sewage systems, implementing a sustainable waste disposal system, and providing pipes for safe water. The provision of safe water, basic sanitation, and hygiene practices is critical to preventing and controlling the transmission of cholera and other waterborne diseases.
In response to the 2023 cholera outbreak in Zimbabwe, the government and non-governmental organizations launched extensive efforts to combat the disease. These combined efforts appear to be working, but more effort will be needed to get to zero cases. MSF continues to support cholera response around the country.
Caring for patients and enhancing cholera prevention measures are both critical elements to bringing the outbreaks under control. But without meaningful action to ensure people’s access to safe drinking water, cholera is likely to resurface regularly in the country.
“If we can convince people to partake in prayers, then surely we can convince them to change their mindsets regarding these diseases.”
MUTARE, Zimbabwe – A traditional healer since 1985, Casemore Darare is all too familiar with medicinal herbs. His services are highly sought after in his neighbourhood of Dora Dombo, a rural area on the outskirts of Mutare city.
But regarding cholera or polio, the 54-year-old has a robust solution: he encourages his community and faith members to strictly get vaccinated, maintain good hygiene, and seek modern medicines at the local clinic when symptoms show.
Casemore Darare, a traditional healer, addresses a meeting of interfaith leaders held in Mutare to discuss cholera mitigation measures
“That’s the most effective solution. There is nothing better, trust me,” he said to loud cheers from participants at a March meeting to develop community-led solutions to address the behavioural and social drivers of cholera and polio.
Darare, the provincial secretary of the Zimbabwe National Traditional Healers Association for Manicaland Province, speaks from experience.
A recent outbreak of cholera that struck him forced Darare to change his thinking about how best to tackle the disease.
After showing symptoms of cholera, Darare said he resorted to what he knew best – traditional medicine.
“I dug up all the herbs I thought could help and mixed some concoctions. I did all the spiritual things I thought would ease my condition. It only got worse,” he said.
Eventually, neighbours put him in a wheelbarrow and rushed him to the nearest clinic, where he received medication from nurses.
“I survived to tell the story. Many people who tried the traditional herbs and spiritual ways were not so fortunate,” said Darare, who enrolled in essential community health training after the ordeal.
Darare is still a traditional healer. But he has also taken up another task of becoming a community champion to encourage people to rely on modern medicines, safe water, sanitation, and hygiene practices to fight diseases such as cholera and polio.
He also encourages fellow traditional healers in his area to immediately refer cholera patients to a medical facility for treatment.
In March, Darare was among the interfaith leaders who gathered in Mutare city to collaborate on how best to fight cholera and polio.
Organised by Apostolic Women Empowerment Trust (AWET)and supported by UNICEF, the gathering brought together traditional healers, leaders of various Christian denominations, and the Muslim faith to collaborate and devise ways to use their influence to drive behaviour change.
Despite their different spiritual doctrines, they agreed on one overarching message of promoting the uptake of vaccines and other modern medicines and practices to combat cholera and polio.
“Cholera and polio do not discriminate. They affect all of us the same. So, we must work together to deliver the message to the people we lead. Some behaviours must change, and we should lead that campaign,” said Sheik Ishmail Duwa, president of the Supreme Council of Islamic Affairs in Zimbabwe.
The meeting timing was critical as the country grapples with the twin outbreaks of cholera and polio, often affecting poor sanitation and hygiene areas.
The meeting also came as Zimbabwe prepared to roll out a second round of mass polio vaccination of children aged ten years and below following a successful first round of polio vaccinations targeting 4.6 million children.
Leaders of apostolic sects present at the meeting pledged to campaign amongst their members to allow children to get vaccinated and for people to embrace modern medicines.
The desire among the interfaith leaders to work together was palpable during the meeting.
They sometimes broke into various small interfaith groups to discuss the causes of cholera and polio, the main drivers, such as open gatherings with no sanitation and hygiene and traditional funeral rites, and how best to address the situation.
Interfaith leaders recently in Mutare to discuss cholera mitigation measures
A Roman Catholic sister stood beside a female traditional healer and Muslim youth leader in one group. A Pentecostal pastor took notes on a flip chart as they engaged in rigorous debate to develop a common position.
Representatives of the groups then presented their findings to a plenary before drawing up a joint action plan that put vaccination, modern medicines and safe water, sanitation, and hygiene practices at the centre of the fight against cholera and polio.
“This kind of interfaith dialogue helps build trust. By learning from each other, we remove the barriers that stop us from collaborating. Cholera and polio don’t need us to follow the old ways of doing things; we must be dynamic and assist the authorities,” said Brian Nemakanga, a leader with the hugely popular Johanne Marange Mafararikwa apostolic sect.
Belinda Magida, a traditional healer, added, “Together, we can influence millions of people in all the hard-to-reach places where we have followers. If we can convince people to partake in prayers and believe in God, we can surely convince them to change their mindsets regarding these diseases. Let’s take the information to the people; let’s positively use our influence. It is a duty we owe to the nation as responsible leaders. Education is key, and knowledge is power.”
UNICEF and WHO, in collaboration with the Ministry of Health and Child Care and funded by the Government of Japan, the multi-donor Health Resilient Fund (comprising contributions from the UK Government, Irish Aid, European Union, and Gavi), and with implementation support from the Apostolic Women Empowerment Trust (AWET), are jointly spearheading diverse Risk Communication and Community Engagement (RCCE) initiatives to address multi-hazards, encompassing efforts against polio and cholera outbreaks.
To avoid complacency and cholera outbreak recurrence, Community Health Promoters encourage safe water, sanitation and hygiene practices
Chitungwiza, Zimbabwe – Many people in Chitungwiza town’s St Mary’s suburb have received the cholera vaccine, in large part thanks to mobilisation efforts by community health promoters such as Ellen Nhambura.
But, even as infections show signs of receding, Nhambura and her team are still moving from house to house to keep people safe.
“We managed to get people to accept the vaccine despite pockets of resistance. Our mission is to teach them to continue practising healthy behaviour after getting vaccinated. The vaccination period is a critical moment because people may relapse into thinking that the vaccine is a replacement for safe and healthy behaviour,” said the 39-year-old who has been a community health promoter for three years.
The Ministry of Health and Child Care, in partnership with UNICEF and the World Health Organisation (WHO), launched a vaccination campaign against cholera on January 29.
The campaign targeted 2.3 million people.
According to the Ministry of Health and Child Care, 2,099,497 people had been inoculated as of February 20, 2024, which signals broad acceptance of the Oral Cholera Vaccine and the success of the campaign.
But vaccination is only part of the response by the government and its partners such as UNICEF.
At the vaccination campaign’s launch, Health and Child Care minister Dr Douglas Mombeshora and UNICEF country representative Dr Tajudeen Oyewale warned against post-vaccination complacency.
They emphasised that while vaccines work, they are not a replacement for safe water, sanitation and hygiene practices that are key to eradicating conditions that cause cholera.
Social and behaviour change campaigns driven by health promoters underpin the efforts to adequately prevent a recurrence of waterborne disease outbreaks.
This involves health promoters such as Nhambura fanning out across communities to raise awareness for people to change their attitudes towards water, sanitation and hygiene issues and share knowledge on effective practices to keep cholera at bay.
On a recent day, Nhambura joined about a dozen other health promoters to traverse the length and breadth of St Mary’s, one of the suburbs affected by the cholera outbreak.
One used a loud hailer to broadcast messages.
They carried and distributed leaflets on the streets and stopped at vegetable markets, shopping centres and bus termini to discuss water, sanitation and hygiene practices necessary to prevent the spread of cholera.
In one street, a group of women and men trooped out of their houses with their children to interact with Nhambura’s team.
Because the area lacks reliable running water, the health promoters emphasised the need for residents to fetch water from safe sources, keep it in clean containers and treat it with water purification tablets or by boiling it before drinking.
Residents listened attentively and asked questions as Nhambura used a flip chart with messages and illustrations on water treatment and storage, toilet and household hygiene, safe food handling, refuse management, oral rehydration and the importance of seeking treatment early.
“I know you are vaccinated, but for a permanent solution, please do these things we are teaching each other here,” said Nhambura, going through pages of the flip chart laden with colourful images of water, sanitation, and hygiene.
Paidamoyo Mhandu (27), one of the residents, said she ensured she and her three-year-old daughter were vaccinated when mobile vaccination teams moved around the area.
She said witnessing some fellow residents falling sick or dying from the disease, as well as the encouragement from health promoters, motivated her to get inoculated.
“But I was no longer treating our drinking water; I thought it was no longer necessary since we had been vaccinated. These health promoters opened my eyes,” she said, reading a flier on cholera prevention.
Community Health Promoters are a vital cog in the health delivery system because of their interpersonal links with communities, said Gertrude Zhakata, the Sister-in-Charge at the St Mary’s Cholera Treatment Centre, where two tents provided by UNICEF have ten beds each to cater for cholera patients.
“These campaigns would not be successful without the assistance of community health promoters. They are the people on the ground; they live within the communities they serve; so, people trust their word. They are a vital bridge between us and the people,” said Zhakata.
She said the health promoters undergo regular refresher courses to keep them updated on disease surveillance and control trends.
The dedication to saving lives beyond the vaccination campaign is palpable as Nhambura and her team move around the suburb wearing sun hats or carrying umbrellas to shield themselves from the searing heat.
She is part of a team of 25 community health promoters who collaborate with the Ministry of Health and Child Care and Oxfam, a partner of UNICEF in Chitungwiza.
They usually leave their homes around 8am to make rounds in the suburbs.
They often return home late in the afternoon after walking between 10 and 15 kilometres and reaching about 200 households daily.
“Yes, it seems like a tough job. But we are a dedicated group, and we know the importance of this work, especially for women and children, because they are the most vulnerable. We do our best to help them stay safe,” said Nhambura.
According to authorities, the door-to-door campaigns have reached over 300,000 people in Chitungwiza town alone.
In Chitungwiza, like other areas across the country, community health promoters are part of a wider more comprehensive social behaviour change campaign that includes radio programmes, road shows, water point committee training and the establishment and promotion of school health clubs.
UNICEF’s cholera response is funded by multiple donors, including the Centres for Disease Control and Prevention (CDC); the European Civil Protection and Humanitarian Aid Operations (ECHO); the Health Resilience Fund (HRF), a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; Japan; the UN Central Emergency Response Fund (CERF) and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from United Parcel Service (UPS) Foundation.
Empowering Communities: Ensuring access to safe water and promoting public awareness on cholera prevention
Zimbabwe is currently grappling with a cholera outbreak, with more than 22,000 recorded cases and over 500 suspected and confirmed deaths.
The widespread impact of the outbreak has touched every corner of the country.
UNICEF is actively supporting the government-led response to the cholera crisis on multiple fronts, treatment of cholera-infected people, initiatives to provide access to safe water, disseminating preventive messages, and advocating for seeking medical support in case of infection.
To address the urgent needs of affected communities, UNICEF supplies critical items such as water purification tablets, hygiene kits, soap, and water containers.
These essentials play a crucial role in ensuring communities have access to clean water and can uphold proper sanitation practices.
Additionally, UNICEF is actively involved in the cholera vaccination campaign and the implementation of public awareness activities, designed to inform communities about cholera’s causes, preventive measures, and the significance of hygiene practices.
Emphasising community participation, UNICEF collaborates with local leaders, influencers, and health workers to effectively communicate key messages and engage communities in the prevention and response efforts against cholera.
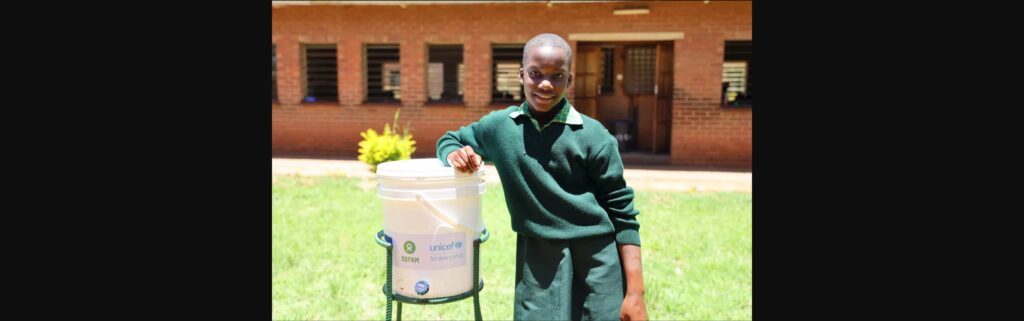
A Learner from Glen View 7 primary school in school in one of the cholera hotspots in Harare is washing their hands using UNICEF supported handwashing station
More than 260,000 people have been reached with critical WASH [water, sanitation and hygiene] supplies, including the distribution of over 1,200 handwashing stations in schools in hotspot areas as part of the back-to-school campaign.
The supply of non-food items (NFIs) ensures that children learn in a safe environment to promote access to quality education.
A learner from Glen View 7 Primary School, in school in one of the cholera hotspots in Harare, standing beside UNICEF supported handwashing station
As part of the back-to-school campaign over 10,000 school children were the recipients of key hygiene messages on cholera and its prevention via Rapid-Pro.
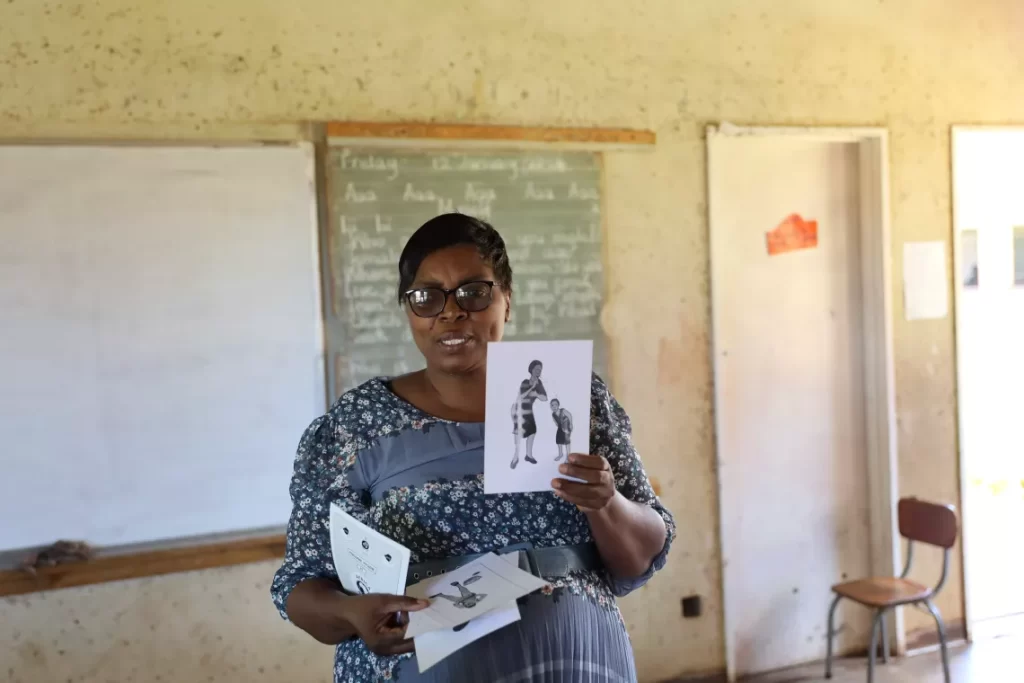
Priscilla Chimbwanda (56), School Health Coordinator uses visual cards to deliver key messages on hygiene messages and Cholera prevention to a classroom full of students
School Health Coordinators have been integral to the back-to-school activities, trained by UNICEF and partners in collaboration with the Ministry of Primary and Secondary Education on essential hygiene messages for cholera prevention.
This ensures a comprehensive approach to addressing cholera within the school environment.
A Community Health Promoter from Glen View, a cholera hotspot area in Harare, delivers door-to-door campaign to deliver key hygiene and cholera prevention messages and the distribution of critical supplies
Community Health Promoters are conducting door-to-door campaigns delivering key hygiene and Cholera prevention messages and the distribution of critical supplies.
UNICEF in collaboration with the Ministry of Health and Child Care, trained over 2,2200 health workers, including Community Health Promoters on household case management, community disease surveillance and treatment of patients.
Health workers play a crucial role as a link between the community and the ongoing efforts.
Pepukai Moyo (21) receives Oral Rehydration Solution (ORS) for her 9-month-old son from Oral Rehydration Point in Kuwadzana, a Cholera Hotspot area in Harare.
The Ministry of Health and Childcare, UNICEF and partners established more than 90 oral rehydration points in hotspot communities nationwide, for rehydration of suspected cholera cases to reduce fatality.
Mothers and their small children, pregnant women, people with disabilities, the elderly, and the chronically ill can now readily interact with facility in community.
Community Health Promoter holding water guard chlorination and litmus paper to conduct testing of household water chlorination levels.
As part of ongoing efforts in the Cholera response, UNICEF and partners capacitated and equipped Community Health Promoters to conduct free residual chlorine testing.
UNICEF is promoting household chlorination to increase access to safe water.
Community Health Promoter, Perpetua Maposa (60) from Kuwadzana, a Cholera hotspot area in Harare, conducts bucket chlorination at a community borehole.
To promote access to safe water, UNICEF has facilitated chlorination of water being collected at community boreholes through Community Health Workers.
More than 200 000 litres of water collected at community boreholes in cholera hotspot suburbs in Harare was made safe through the bucket chlorination approach.
Yvonne Mataranyika (73) receives oral rehydration solution at the Oral Rehydration Point (ORP) in Kuwadzana, a Cholera hotspot area in Harare
UNICEF’s cholera response is funded by multiple donors, including the Centre for Disease Control and Prevention (CDC); the European Civil Protection and Humanitarian Aid Operations (ECHO); the Health Resilience Fund (HRF), a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; Japan; the UN Central Emergency Response Fund (CERF) and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from Universal Postal Services (UPS).













































Recent Comments