HEALTHCARE professionals have raised a number of issues which they say were not captured in the proposed Medical Services Amendment Bill.
The medical professionals say they want the State to clearly outline its obligations with regards to reimbursement for services rendered by private health care providers as the clause on fee payment, which is the proposed section 12A (2), “is vague and may need further clarification on how it will be implemented”.
This is contained in a statement by some the human rights doctors following a petition they presented to the Parliamentary Portfolio Committee on Health and Child Care.
The Zimbabwe Association of Doctors for Human Rights (ZADHR) said it came up with the petition after conducting physical meetings across the country and on X spaces.
“The reimbursement model, where government reimburses for services rendered, is not working effectively, local authorities are owed huge sums of money by government. Private institutions are businesses and cannot afford to have funds locked up for inordinate periods,” the rights doctors said.
They added: “Private healthcare providers appreciate a clear payment arrangement or even fiscal incentives like rebates or tax credits. This will ensure that these institutions are properly resourced and their staff is motivated enough to deal with any medical emergency. There is need for further detail to bring clarity.”
ZADHR also said the 48-hour minimum admission clause is a cause for deep concern, this is in reference to the proposed section 12A(1) of the Bill.
“Prescribing minimum hours for patient stabilisation is problematic and this could have been a transcription error by the authors, hence it needs to be corrected and addressed. In most cases, stabilisation won’t take long and this may become expensive for the patient if they are asked to foot their own bill, or even the State,” they said.
They also raised concern over the pegging of fees by the Health minister, as in clause 8 of the Bill, saying this was tantamount to micro-management.
“Operational issues should be left to technocrats. Instead, the Bill should create an advisory panel to work on the general principles rather than drawing the minister to set fees. Involving the minister in such operational issues will affect the turnaround time given the hyper-inflationary environment,” the rights doctors said.
In its Bill Watch edition yesterday, legal watchdog Veritas also raised concern saying “the new powers the Bill will give to the secretary for Health will have to be administered with a light touch if they are not to stifle the provision of healthcare by the private sector”.
“For example, private health institutions could be overwhelmed if too many patients are transferred to them from government hospitals and as we have said, it is not clear that the State will reimburse the private institutions for the cost of treating those patients,” Veritas said.
“There is some lack of clarity in the new Bill for example the definition of ‘basic healthcare’ is meaningless but generally, the Bill succeeds in its stated aim of bringing the Act in line with the Constitution.
“That said, bringing the Act in line with the Constitution is not the same as providing healthcare of a standard envisaged by the Constitution. Raising the standard of healthcare in Zimbabwe will not be achieved by simply amending the Act: it will entail rehabilitating our hospitals, clinics and health institutions, and increasing the professionalism of our healthcare providers. All of which will require money which the government does not provide.”
Community health worker Maria Matuka didn’t grow up riding a bicycle – but now she considers it indispensable to her life-saving job.
Maria Matuka’s job as a community health workers is made easier by a bicycle built for the rugged roads in Chiredzi, Zimbabwe
MARIA Matuka arrives at Chizvirizviri Clinic, in Chiredzi, south-east Zimbabwe, to collect the medical supplies she will distribute in the village.
Looking physically fit, the 46-year-old mother of four has cycled more than five kilometres from her home to get to this health facility – her nearest clinic, and the only one for a long way in this sparsely populated area.
The roads are rugged and the terrain is rough, making it difficult to access even in an off-road car.
While cycling is a popular leisure-time physical activity in some parts of the world, in this remote part of Zimbabwe, it is not only a crucial form of transportation, but a lifesaver.
“If you reduce the distance to a few kilometres, the mothers will bring their children [for vaccination].”
– Simbarashe James Tafirenyika, president of the Zimbabwe Municipalities Nurses and Allied Workers Union
Sitting tall on a black saddle, Matuka visits households to talk to mothers about getting their babies vaccinated against risky infectious diseases like tetanus, measles and poliomyelitis.
“It takes some minutes to move from one household to another, encouraging mothers to bring their babies to a centre in the village for vaccination,” Matuka tells VaccinesWork.
“It was difficult when I became a village health worker without a bicycle. It was draining. I felt cramp pains and numbness after walking long distances.”
Matuka is one of the 45,923 community health workers in Zimbabwe provided with bicycles at no cost since 2009 by World Bicycle Relief (WBR), a charity based in the United States.
Maria Matuka, a vaillage health worker, reports every month at Chizvirizviri clinic
Getting closer
Zimbabwe’s Expanded Programme on Immunisation (ZEPI) has been making routine vaccines available for free to children since 1982, initially to beat back illnesses including measles, polio, tetanus, tuberculosis and diphtheria.
Over the years, the programme has grown to protect against other diseases, such as Hepatitis B.
Matuka became a community health worker in January 2021 and got her bicycle in December of the same year. It was her first time owning and riding a bike, and it took her a few days to learn, with lessons from her neighbour’s children.
But challenges, including logistical hurdles, mean there’s still further to go on coverage.
Matuka says some rural communities live long distances away from a health facility, a factor which has a negative effect on health-seeking behaviours.
“This is why we have a baby clinic every month,” she says, referring to an outreach campaign in which mobile clinics manned by nurses bring vaccines closer to children not only in rural areas, but urban areas too.
This initiative, and the bicycles, help health workers like Matuka take health services to the people.
“If you reduce the distance to a few kilometres, the mothers will bring their children [for vaccination],” says Simbarashe James Tafirenyika, president of the Zimbabwe Municipalities Nurses and Allied Workers Union, a labour union that represents nurses employed by local authorities.
A bridge between the health system and the community
The Health Ministry also rolls out vaccination campaigns for children against diseases like measles and polio, when the need arises.
For instance, in 2022 and 2023, Zimbabwe undertook nation-wide supplementary immunisation activities with bivalent oral polio vaccine following the detection of wild poliovirus 1 in neighbouring Mozambique and Malawi in 2022.
Village health workers like Matuka play a critical role in interventions like these through mobilisation of mothers in rural areas, who can often fall beyond the reach of professional health workers.
“Currently, the village health workers move around communities conscientising mothers and disseminating information to them,” Tafirenyika says.
“Some people in the rural areas have no access to radios and television, which often broadcast information on vaccines. It is village health workers who disseminate information about national immunisation programmes.”
Matuka became a community health worker in January 2021 and got her bicycle in December of the same year.
It was her first time owning and riding a bike, and it took her a few days to learn, with lessons from her neighbour’s children.
“I grew up in Zaka and our culture and tradition did not allow women to ride bicycles,” says Mutuka, recalling her memories from her rural home in Masvingo province.
She not only educates mothers about vaccination, but also passes on other knowledge and skills.
“I mobilise mothers to come for monthly baby weighing. I also educate them about breastfeeding as well as monitoring the health of their babies using the mid-upper arm circumference (MUAC) tapes,” she says, referring to a measurement that is used to quickly determine if a child is acutely malnourished.
“I also test people for malaria and recommend them to visit the clinic for further diagnosis. I also collect from the clinic and distribute medication to people living with human immunodeficiency virus (HIV) and tuberculosis (TB).”
Matuka, who reports every month at Chizvirizviri Clinic, distributes pamphlets on different health issues like malaria and cholera prevention to people in the villages.
Tafirenyika says she plays a crucial role in educating people in remote areas.
“Some people do not know the importance of these vaccines which are given to children. The pamphlets can help some people who can read to know the importance of those vaccines and how they help in curbing and preventing highly infectious diseases like polio,” he says.
Sean Granville-Ross, Executive Director of Programs at World Bicycle Relief, says village health workers are essential in delivering health care services to rural communities, where access to health care facilities can be limited due to distance.
“These health workers provide vital services such as vaccine mobilisation, maternal and child health care, nutritional education and basic medical care. However, without reliable transportation, their ability to reach patients is severely restricted,” Granville-Ross tells VaccinesWork.
“A Buffalo Bicycle allows them to cover much more ground – reaching up to 88% more patients, quadrupling the frequency of patient visits and allowing health workers to spend more time with patients. This significantly enhances their ability to ensure that mothers in rural areas are informed and motivated to vaccinate their children, helping to improve health outcomes across the community.”
One of the shops where village health workers get parts to service their bicycles in Chiredzi town
Calls to increase remuneration for village health workers
Village health workers are registered with the local clinic and the Ministry of Health and Child Care.
Some are given allowances from various development partners they work with, but experts and labour unions say more needs to be done to remunerate – and incentivise – these essential health workers across the country.
Itai Rusike, the executive director for Community Working Group on Health (CWGH), says village health workers should be supported with allowances from the national budget to enhance their work and motivate them, instead of the current situation where they rely on external partners for their tools of the trade.
“At the present there is no standardisation of payment of allowances. Some are paid their allowances on time, with others not being paid on time,” Rusike tells VaccinesWork.
Matuka’s bicycle is regularly serviced at a low cost at a workshop near Chizvirizviri clinic by a mechanic trained by the American charity.
Plans are underway to expand the programme to additional districts to scale efforts to improve health care access and support national vaccination initiatives in rural communities throughout Zimbabwe, says Granville-Ross.
Matuka says she wishes the bicycle could be modified to have a luggage carrier to ferry medical supplies and educational materials.
“Currently, I carry a heavy bag with the supplies on my back, which is painful,” she says.
Sanele Mutsiwa with daughter Faith at Kezi Rural Hospital
SANELE Mutsiwa, 25, smiles at her two-year-old daughter Faith at Kezi Clinic in Matobo district, Zimbabwe, where she has gone to get her child vaccinated.
She holds a baby card, while Faith sits on her lap.
Sanele says she owes this happy moment to her local village health worker, who supported her during pregnancy and after birth.
It was village health worker Duduzile Ndlovu who conducted Sanele’s pregnancy test, encouraged her to make the 3km journey to the hospital to make a booking, and continued to monitor the mother and baby after birth.
“Duduzile has been with us all the way,” Sanele says.
“She makes sure I know about the nutritional needs of my child, informs me about disease outbreaks and immunisation campaigns and pushes all of us in the community to adopt safe water, sanitation and hygiene practices.”
Sanele lives in Matabeleland South province, a poor rural region of western Zimbabwe, where it is difficult for young mothers to reach a health facility and have their babies vaccinated.
But now they can rely on village health workers who come and reach out to them, where they live.
In the arid landscapes of Mangwe and Matobo districts, the sight of a village health worker in her distinctive smock uniform and brown hat, pedaling down dusty paths on a blue bicycle with a China Aid logo, has become a beacon of hope.
For 60-year-old Ottilia Ncube, a village health worker in Mangwe with its scattered villages and homes, this simple mode of transport has revolutionised her ability to bridge the gap and deliver vital healthcare services to her community.
Ottilia’s bicycle is more than just a means of transport — it’s a lifeline.
“Home visits were a nightmare before I got this bicycle. I would walk, but there were areas I simply couldn’t reach,” she says.
“The bicycle is an answer to my prayers.”
Otilla Ncube with her bicycle, distributed by the Ministry of Health and Child Care, with support from UNICEF and China
On a typical day, Otilla packs her maternal and neonatal care equipment and sets off on her bicycle to visit households in the community.
Under a grass-thatched gazebo, she sets up her equipment.
Ncube’s role extends beyond health checkups.
She is also a crucial link in promoting safe water, sanitation and hygiene practices.
During her home visits, she inspects homes and ensures that families are following proper hygiene practices, such as treating and storing drinking water safely.
She also teaches mothers and their children how to properly wash their hands.
“At community level, the village health workers have been trained to identify danger signs in mothers and their newborns and make referrals to the health facility,” explains UNICEF Zimbabwe health specialist Meggie Gidiba.
Reducing child deaths
This crucial support is part of a broader initiative by the Ministry of Health and Child Care, in partnership with UNICEF and funded by the Government of China.
Between 2018 and 2020, 600 bicycles were distributed to village health workers across Matabeleland South and Mashonaland Central provinces.
The goal was to improve access to maternal, newborn, and child health services in these hard-to-reach areas and to enhance the quality and use of these services.
Along with the bicycles, village health workers received kits equipped with essential tools such as respiratory timers, mid-upper arm circumference (MUAC) measuring tapes, weighing scales, thermometers, and medical supplies.
These tools are vital for monitoring the health of pregnant women, newborns and children under five, and for ensuring timely interventions.
The programme is making a crucial contribution to Zimbabwe’s efforts to meet UN Sustainable Development Goal (SDG) 3, which aims to reduce neonatal mortality in all countries to at least 12 per 1,000 live births by 2030.
Zimbabwe still has a significant way to go to reach the Goal. In 2019, neonatal mortality rate stood at 32 deaths per 1,000 live births.
The numbers had not significantly changed since 2010.
Against this background, however, the UNICEF and China’s support to village health workers is paving the way for important progress.
According to the district nursing officer for Mangwe, Ncebile Ngwenya, the programme has already gone a long way in improving access to health care in remote areas.
“We now have good linkages with our communities. We are leaving no one behind,” she says.
Otilla and Juliet Ncube conduct a routine check of Daphne and her daughter Priscilla in a grass thatched gazebo
Community outreach
Another village health worker to receive UNICEF training is Duduzile Ndlovu from Matobo district – the one who visited Sanelle when she was pregnant.
Duduzile was among 3,500 village health workers who received a refresher training in 2021, as part of the China-funded initiative.
This focused on community-based surveillance and home management for mothers, newborns, and children under five.
Midwives and doctors also received on-the-job mentoring and capacity building in basic emergency obstetric and newborn care.
Duduzile says she is now better equipped to engage people in her community, including those previously resistant to modern medicine.
“The training really upgraded my skills. I understood that it is important to avoid home deliveries at all costs,” she emphasises.
Before, the local clinic registered several home deliveries each month, a risky practice that often leads to complications.
“We used to record about four home deliveries a month, but we have been recording none since the training,” says Hazel Moyo, a primary care nurse at Kezi Clinic.
According to Hazel, diarrhoeal diseases are now also managed better.
“Sometimes parents would bring children when it was too late to save the child’s life,” she continues.
“The village health workers didn’t know much about diarrhoea, but they can now identify cases and administer oral rehydration salts.”
Medical supplies, funded by China, at Embakwe District Clinic in Mangwe District
Support from China
Zimbabwe is one of 22 countries so far across Africa and Asia to receive funding from the Government of China, through CIDCA, for UNICEF programmes for children.
Zhou Ding, China’s ambassador to Zimbabwe, highlights the achievements of the programme.
“Cumulatively, 1,74 million people were reached, including pregnant women, children and families,” he says.
Over 57,000 pregnant women were referred to health facilities, and 447,138 children under five received growth monitoring services.
Additionally, village health workers treated 5,216 children with diarrhoea using oral rehydration salts and zinc in their communities, a significant achievement in preventing child mortality.
“I learned that immunisation helps to ensure a child’s health, and if I don’t come my child could have health problems,” mother Masleen Mabikire explains while her daughter, six-month-old Melina receives a vaccination drop.
The girl looks happily at her mother, her mid-upper-arm circumference standing at healthy 13.5 centimeters, which indicates an appropriate nutritional status.
In Beijing, UNICEF China Chief of Public Partnerships Sae-Ryo Kim stresses that “China has made remarkable progress on children’s issues in the last four decades. It can now support other countries in their development. That’s why UNICEF and the Government of China are working together to support children in more than 20 countries around the world, including Zimbabwe.”
For children like Faith and Melina, this support from UNICEF and China means that they can now look forward to a brighter and healthier future.
A LEADING disease monitoring agency has declared a public health emergency across Africa, including Zimbabwe, following the outbreak of Mpox, a highly infectious disease previously known as monkeypox.
Scientists from the Africa Centres for Disease Control and Prevention (Africa CDC) say the new strain of Mpox is spreading at an alarming speed.
According to the latest quoted statistics, since the beginning of 2024, more than 13 700 cases and 450 deaths have been recorded in the Democratic Republic of Congo (DRC), a country which many Zimbabweans, mostly truckers, visit on business.
According to the latest epidemiological trends, including an update on the geographic expansion of Mpox in the World Health Organisation (WHO) African Region (July–August 2024), the disease is readily spreading across the continent.
Speaking during a live Press conference Tuesday, Africa CDC director-general, Jean Kaseya officially declared the ongoing Mpox outbreak a public health emergency and urged stakeholders to collaborate and safeguard the security of millions of people.
“This declaration highlights the urgency and gravity of the situation, demanding immediate and coordinated action across Africa. We are mobilising all available resources, working closely with Member States, strengthening partnerships, and intensifying efforts to contain and mitigate the impact of Mpox,” Kaseya said.
The virus, which causes lesions across the whole body, has reportedly spread to other African countries, including Burundi, the Central African Republic (CAR) Kenya and Rwanda.
The declaration of a public health emergency helps governments coordinate their response and potentially increase the flow of medical supplies and aid into affected areas.
Kaseya warned that the disease could spiral out of control if immediate steps were not taken to contain it.
“This declaration is not merely a formality. It is a clarion call to action. It is a recognition that we can no longer afford to be reactive. We must be proactive and aggressive in our efforts to contain and eliminate this threat,” he said.
Kaseya said there were plans to secure about 10 million doses to limit the spread of the outbreak in Africa.
According to research, there are three vaccines available to prevent Mpox but only persons at risk, or who have been in close contact with an infected person, are usually vulnerable.
Mpox spreads from animals to humans and between people through close contact with someone who is infected, including through sex, skin-to-skin contact and talking or breathing close to another person.
It can cause symptoms such as fever, muscle aches and lesions across the body. If left untreated, Mpox can be deadly.
HARARE – The Health and Child Care ministry , with the support of the World Health Organization, and other partners has immunized over 200,000 people against cholera in the most vulnerable communities.
This campaign has reached 22 wards in eight districts: Chegutu, Chiredzi, Chitungwiza, Masvingo, Mhondoro-Ngezi, Mutare Rural, Mt Darwin, and Sanyati.
These targeted areas, have high artisanal mining activities where access to safe water and sanitation facilities is limited.
In these communities, clean water is scarce and health risks are high.
Hence, the vaccination campaign has brought great relief.
This initiative is beyond the numbers; it’s about saving lives and securing a healthier future.
“We remain vigilant in our efforts to strengthen our health systems and build resilience against future outbreaks,” said Health and Child Care cholera incident manager Dr Isaac Phiri.
Pelagia Chikoore, a 51-year-old resident of Venice Mine, Mhondoro Ngezi, emphasised the importance of the vaccine.
“l got vaccinated to prevent myself from getting cholera,” she said.
“Our area has a lot of mining activities, and sometimes water supply is a challenge. Although we now have a solar-powered borehole, I believe the vaccine is an extra layer of protection.”
While vaccination is not a silver bullet, it provides an additional layer of protection, especially in areas with limited access to clean water and sanitation.
Echoing Chikoore’s sentiments, 21-year-old Alice Mhembere from Mubaira shared her experience. “l know the vaccine protects me from cholera,” she said.
“We saw people getting sick because of cholera so I never hesitated when I got the opportunity.”
Cholera is a highly contagious disease that spreads through contaminated water and food.
By administering vaccines, the campaign helps to build immunity in populations at high risk, reducing the likelihood of disease spread and protecting communities from potential outbreaks for a period of 6-12 months.
Hence, it needs to be complemented by improvements in water supply and sanitation infrastructure to ensure communities are protected from another episode of cholera outbreak that claims innocent lives.
WHO played a crucial role in combating a cholera outbreak in Zimbabwe.
With unwavering commitment, WHO supported two rounds of targeted vaccination campaigns, providing the technical guidance and logistical support needed for success.
The vaccination campaigns were not only effective but also efficient, achieving over 90% coverage, and reaching the people who needed it most and making a significant impact on the community’s health.
The vaccination campaign was made possible through funding from the International Co-ordinating Group (ICG), GAVI, the Vaccine Alliance and WHO.
This collaborative effort brought hope and relief to many, showcasing the power of unity and expertise in the face of a health crisis.
“We are proud to have supported Zimbabwe in this crucial vaccination campaign. By reaching out to most vulnerable communities, we are not only preventing disease transmission but saving many lives,” said Dr Desta Tiruneh, WHO representative to Zimbabwe.
Zimbabwe’s latest cholera outbreak swelled to more than 20,000 suspected cases, but nurses and health leaders say the new, easy-to-use, rapid screening kits will make the fast-spreading infection easier to manage in future.
In the wake of a cholera outbreak that has ravaged both rural and urban communities, Zimbabwe health workers say new cholera rapid diagnostic tests (RDTs) are proving to be a game-changer.
The introduction of cholera RDTs in Zimbabwe is part of a global initiative spearheaded by Gavi, UNICEF, the World Health Organization and FIND, and will see over 1,2 million tests being distributed to 15 high-risk countries.
Previously overwhelmed by the demands of traditional cholera testing, health professionals across Zimbabwe say their workload has been reduced. After kits arrived in Harare in April, the use of RDTs is now in full swing across the country.
“The introduction of the RDTs has allowed us to diagnose suspected cholera cases within minutes. In the past we would wait for lab test results to determine whether a patient is negative or positive. The kits have helped in the containment of the disease,” said Anasia Mutero, a senior nurse at a rural clinic in Buhera district, the epicentre of the 2023–2024 cholera outbreak.
Stephen Sithole, another nurse in the district, echoed Mutero’s assertions.
“We can now test patients immediately and after 15 minutes the results will show if they are positive. We then take the correct action, saving time, and also life. The test kits have significantly improved health outcomes,” said Sithole.
Kits in action
A practical demonstration at Harare’s Beatrice Infectious Disease hospital showed the swiftness of the tests.
“Running a cholera rapid diagnostic test is relatively straightforward. The first thing is collecting a stool sample from the patient, which is then mixed with a buffer solution provided in the test kit. Drops from the mixture are added to the test strip and left undisturbed for about 15–20 minutes.
“During this time, the sample travels up the strip. If cholera bacteria are present, specific antibodies on the strip will react and produce a visible line, indicating a positive result. The whole process typically takes about 20–30 minutes from sample collection to result reading,” said Sister-in-Charge Priscilla Chizema during the demonstration.
Saving lives, curbing spread
“Without a shred of doubt, the kits have helped not only in saving lives, but also control of the spread of cholera, as patients can quickly get treatment once detected. Identifying possible cholera cases has significantly reduced the potential for outbreaks,” said Dr Collins Muchemwa, a physician at Harare Central hospital.
Director of Epidemiology and Disease Control and Neglected Tropical Diseases (NTD) in the Ministry of Health and Child Care Dr Isaac Phiri said the RDTs were a game-changer.
“We received 66,000 kits from the Vaccine Alliance [Gavi]. Prior to receiving the kits, nurses from districts and provincial hospitals across the country had undergone trainings. We want every nurse across the country to be trained. The kits are an important tool in the detection of cholera as we can quickly test for cholera in suspected cases and if the results are positive the patient is put under treatment,” said Dr Phiri.
Matron Shamiso Maturure echoed Dr Muchemwa’s sentiments, but emphasised that the kits’ ease of use makes them useful at the primary health level, where restricted technical skill might rule out the deployment of more sophisticated tools.
“[The kits’] simplicity allows our ability to manage patients, reducing the burden on our resources. The RDTs meaningfully improved the capacity to respond to the disease, not only at major hospitals, but also at local clinics,” she said.
CAPTION::Health workers using the new cholera rapid diagnostic tests. Credit: Elia Ntali
“We want every nurse trained”
Since early April, some 986 nurses and 44 laboratory personnel from provincial and district-level clinics have undergone training on the use of the test kits, supported by funding from partners including the Health Resilience Fund, the European Union, the UK, Ireland, Gavi and others.
Chiredzi District nurses Moses Ndaba and Evelyn Tavarwisa were among them. “It was really enlightening: the knowledge that we acquired assisted us in case management – something which we are practising at our stations. I want to believe that the trainings have helped a lot in containing the spread of cholera,” said Ndaba.
“The training we received will go a long way in addressing the cholera-related issues. It equipped me with the knowledge and skills that we are implementing today. The results are there, and we have testimonies that the RDTs have lessened the burden of waiting for days for results,” said Tavarwisa.
According to WHO, prior to the recent arrival of new-generation RDTs, testing capabilities in the country were problematically limited.
“Between the [recent] outbreak’s onset in February 2023 and 18 January 2024, only 2,090 antigen RDTs and 2,250 culture tests were conducted across 10 health centers. Following the training, the number of antigens RDT tests skyrocketed to 9,853, a staggering 371% increase. Culture tests also saw a significant rise, reaching 6,386, reflecting a 184% increase
That growth signifies a fourfold increase in testing accessibility in rural facilities, WHO went on to point out. Empowering nurses to carry out the testing has freed up the time of more specialised laboratory workers.
More than 20,000 suspected cholera cases and more than 400 confirmed deaths were recorded since the detection of the first cholera cases in Zimbabwe last year.
A government-led cholera response, with support from development partners, was rolled out with a focus to streamline response coordination at various levels.
This included prevention and treatment interventions.
In addition, the government embarked on a programme to provide safe water by drilling solar-powered boreholes in the most affected areas.
In Zimbabwe, limited access to basic health services in artisanal and small-scale mining characterises the harsh realities of excessive exposure to silica-containing dust, overcrowding and poor living conditions for miners.
Zimbabwe is currently experiencing a high burden of TB, silicosis and HIV among communities of artisanal and small-scale miners.
Multi-sectoral and innovative actions are required to stem this triple epidemic in Zimbabwe.
The risk of silicosis for people has increased due to the severity of exposure to silica dust.
Our goal is not only to address the immediate health needs of these miners, but also to empower them with the knowledge and tools to protect themselves. — Dr Munyaradzi Sidakwa, Project Medical Manager
Silicosis is a lung disease that comes as a result of exposure to silica, which is found in dust.
The risk factors among subsistence miners have to do with the work they do — digging, blasting and other related activities.
The burden of respiratory diseases affects artisanal small-scale miners, because of various socioeconomic factors like a lack of protective clothing, limited access to healthcare and a lack of knowledge about the diseases and preventive measures they can take when engaging in their operations.
The miners are also exposed to sexually transmitted infections due to the prevalence of sex work in mining communities.
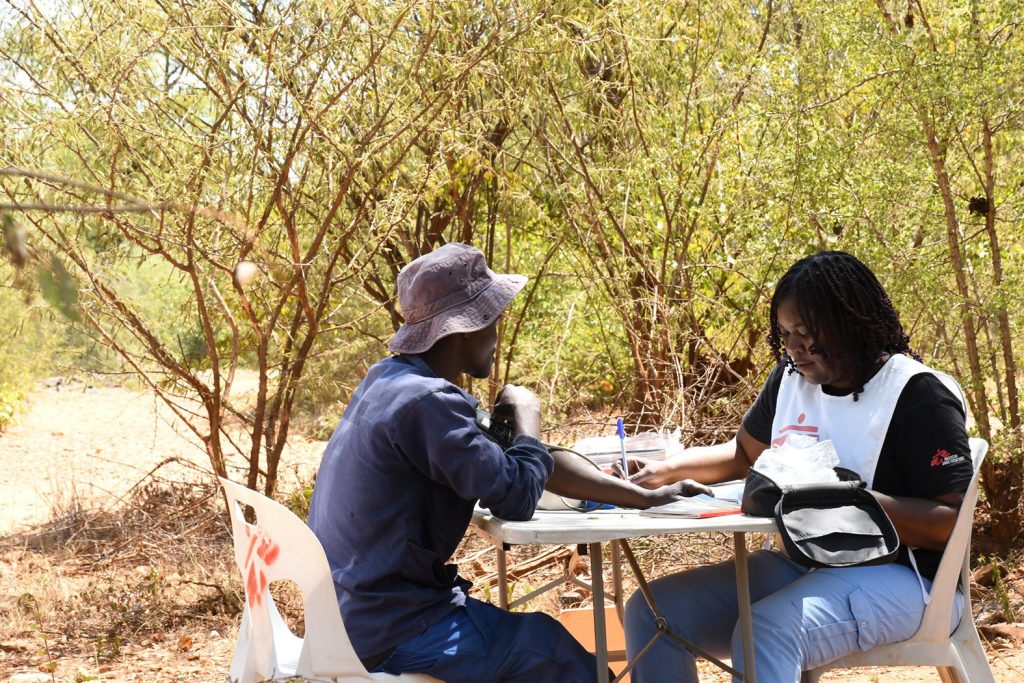
To provide basic healthcare services to the artisanal miners, Médecins Sans Frontières (MSF) is running a medical outreach initiative in Gwanda District, Matabeleland South province, supporting the Ministry of Health and Child Care (MoHCC) in reaching hard-to-reach communities, specifically targeting those occupied in artisanal small-scale gold mining, with a comprehensive basic healthcare programme.
MSF selected Gwanda district for an intervention because of poor health indicators in the artisanal mining community.
CAPTION::An MSF nurse assists and checks the blood pressure of a patient. Zimbabwe, March 2024.
The outreach programme aims to bridge the health services gap and bring essential healthcare services directly to the miners’ doorsteps.
By working hand in hand with the MoHCC, MSF provides access to communicable and non-communicable diseases prevention, screening and treatment.
“We noted some of the main gaps and partnered with the Ministry of Health and Childcare to conduct outreach programmes to artisanal mining sites,” says Dr Munyaradzi Sidakwa, project medical manager.
“Our goal is not only to address the immediate health needs of these miners, but also to empower them with the knowledge and tools to protect themselves and their communities in the long run and the screening is for free.”
Host communities and artisanal small-scale miners in hard-to-reach areas delay seeking medical care.
They do not follow through with referrals; they struggle to adhere to treatment; they also struggle to access affordable care; and they frequently rely on traditional treatments that are readily available and easily accessible.
The miners are also hard to reach with public health information because of their mobile nature; they move from one place to another in search of rich gold deposits.
Distance has been one of the major hindrances to access medical care for miners and host communities, and this has ultimately affected their health seeking behaviour. They have to travel for anything between six and 30km to access the nearest health facility.
”We provide a comprehensive package and address the health challenges being faced by the artisanal miners, which include HIV, TB, and silicosis.DR MUNYARADZI SIDAKWA, PROJECT MEDICAL MANAGER
Meandering through the bumpy roads, MSF teams reach the artisanal mining areas.
The patients will be waiting, heeding the call after a two-day mobilisation by the health promotion team, two days prior to the medical outreach. Women and children are the first to come.
Men trickle in during lunchtime, as they work underground.
Past midday, tired and weary, they join the queue to get screened and medication.
MSF teams, comprising doctor and nurses, pharmacy technicians, and health promoters, organise mobile clinics to artisanal mining sites scattered around Gwanda district to provide medical care, and on some days, they go to host communities.
Clinics are held four days a week, with the teams visiting two different locations per day.
Each day, they attend to new patients, seeing a minimum of 70 patients in the mining locations and over 200 patients in communities.
The medical services include free screening for conditions such as tuberculosis (TB), HIV, cervical cancer screening, hypertension, sexually transmitted infections, and providing family planning services. Medications are provided for free at clinics.
Patients that cannot be treated at a clinic or requiring advanced interventions are referred to Gwanda Provincial hospital.
To date, MSF teams have reached over 4 000 artisanal miners and host communities with mobile clinics.
CAPTION::A child receives treatment consultation from an MSF nurse. Zimbabwe, March 2024.
“It is hard for them to reach the facilities, so, during such programmes, we go to the mining sites,” says Dr Sidakwa.
“We provide a comprehensive package and address the health challenges being faced by the artisanal miners, which include HIV, TB, silicosis, limited access to condoms and family planning methods, STIs, drug and substance use and mental health issues.”
The demand for services is high, with the mining community appreciating the efforts by MSF teams to bring healthcare services closer to where they are.
“I find it hard to visit the clinic, even when I feel sick. During the day, we will be busy in the mining holes, so I better sacrifice to get money to fend for my family. We suffer from the inside with generalised aches and pains but we just ignore them, but chest pains are severe. Now that we are getting medical services here, it is easier for me,” said Amon Ndhlovu, one of the artisanal miners.
Effective control of TB, silicosis, and HIV among miners requires addressing the identified knowledge gaps and barriers that are faced by miners in accessing personal protective equipment and healthcare services.
This will require multi-sector collaboration and the involvement of miners in co-designing a package of healthcare services that are tailored for them.
To ensure sustainable access to healthcare services by artisanal miners, MSF recommends stakeholders to collaborate with MoHCC to ensure that artisanal miners access health services with the establishment of health posts in places nearer to mining communities.
Catherine has dedicated the past eight years to being a community health volunteer because she passionately believes that no one in her community should die from ignorance.
Catherine has dedicated the past eight years to being a community health volunteer because she passionately believes that no one in her community should die from ignorance.
Living in Glen View, a densely populated suburb east of Harare, Catherine balances her roles as a mother and provider with her commitment to volunteer work.
She and her husband work together to support their family of four, but Catherine’s true calling extends beyond her household.
Volunteering allows her to give back and share vital health knowledge with her neighbours.
“I always feel that we should help each other as a community because sometimes people die due to ignorance,” she explains, highlighting her unwavering dedication to improving the well-being of those around her.
Community health volunteers play a vital role in communities as they often are the first point of contact for those seeking medical help or solutions.
In the current cholera outbreak in Zimbabwe, which has affected 34 531 people since February 2023, community health volunteers like Catherine have played a vital role in educating and sensitising communities on prevention and knowledge on what to do should cholera happen.
Catherine said: “I have also been a community health volunteer since 2016 and help the community regarding cholera, a current problem. During this time, we encourage people to drink clean water. Usually, we face water challenges, and people fetch water from unprotected sources. We encourage them to treat their water and properly cook their food.”
From February 2023, 1 614 community health volunteers were trained from all 10 provinces to support cholera response activities in the community.
The cadres reached approximately 1 660 000 people through various engagements, using door-to-door and mass awareness approaches at churches, funerals, markets, and schools.
For Catherine, being a community health volunteer is a passion and a calling.
She manages her time to engage the community on health issues, including the cholera outbreak, and keep her small community business going to support her family.
She highlights key points where she engages the community, such as the water points.
Here, the community collects water at designated times, and she can engage and teach her community on issues of cholera prevention, including hygiene and sanitation and the available resources at health centres.
Community health volunteers support monitoring rehabilitated water points as part of water point committees, benefiting approximately 424 000 people.
“The training at the water point will enable me to provide health education. Some people get sick and do not tell anyone, so they use home remedies. At the water point, we urge them to visit the clinic and get vaccinated.”
UNICEF’s cholera response is funded by multiple donors, including the Centre for Disease Control and Prevention (CDC); the European Civil Protection and Humanitarian Aid Operations (ECHO); the Health Resilience Fund (HRF), a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; Japan; the UN Central Emergency Response Fund (CERF) and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from United Parcel Service (UPS) Foundation.
UNICEF is supporting community-based platforms to ensure children continue to get a diversified and nutritious diet
UNICEF is particularly concerned about the vulnerability of children. Decreased access to clean water and a poor diet heightens the risk of malnutrition and diarrhoeal diseases among children and impacts their rights to education and protection with the full effect of these intersecting factors expected to manifest only later. Hence there is a need for a front-facing preventive strategy to avert excess deaths in the months to come.
UNICEF is urgently appealing for US$84,9 million to fund its emergency response aimed at assisting children and women affected by the El Nino crisis in Zimbabwe.
This funding will provide life-saving interventions to 1,34 million people, including 866 000 children, amidst a complex humanitarian crisis exacerbated by water and food shortages.
As part of its El Nino response, UNICEF is supporting the scaling-up of community-based platforms such as Care Groups to promote life-saving interventions and to contribute to avoiding malnutrition among children.
Zimbabwe is facing the impact of a strong El Nino event which started in December 2023 and has caused above-average temperatures and below-average rainfall, with a “historic” mid-season dry spell.
This El Nino is being compared in severity to the 2015-16 El Nino.
The El Nino induced drought resulted in an extremely poor harvest. Over 60 per cent of the crops planted this season were lost.
The effects of this El Nino are expected to impact child nutrition until well into 2025.
The challenges created by El Nino in Zimbabwe came at a time when the country was also faced with public health emergencies related to cholera and polio, putting Zimbabwe into a complex, multi-dimensional humanitarian crisis.
During the El Nino induced drought in Zimbabwe, a total population of 7,6 million people urgently requires life-saving and life-sustaining humanitarian assistance and protection support, as well as livelihood support, so that they may recover their losses, rebuild resilience, and access basic services.
The drought increases the risk of malnutrition, infectious diseases, maternal complications, and gender-based violence.
An estimated 1,4 million people require nutrition assistance, while 1,8 million learners are at risk of educational disruption due to the drought, potentially leading to increased school dropouts and child protection issues.
A total of 29 high-priority districts – mainly in all the eight rural provinces which include Matabeleland North and South, Mashonaland East, Central and West, Midlands, Masvingo and Manicaland – have been identified at most affected by the drought.
Picture from a farmer in Mudzi District, Mashonaland East Province, which has been impacted by the drought.
The water source for the community garden has completely dried up. Local communities are struggling to get access to food and water.
Most at-risk populations of the El Nino induced drought are children under five years, pregnant and lactating women, and adolescents.
CAPTION:A group of ladies who form a care group, run by a community-based lead mothers, deliver a holistic package of counseling and support.
UNICEF is working with the Government and partners to protect diet diversity and child feeding practices and to avert a rise in child malnutrition.
UNICEF and partners are expanding and strengthening the national multi-systems community-based model for the prevention of all forms of malnutrition, with care groups as the delivery platform.
Care groups, run by a community-based lead mother, deliver a holistic package of counseling and support including for health, nutrition, child development, water, sanitation and hygiene, and are linked to other forms of support available in the district including social protection (cash and food distributions), agricultural support and income generation activities.
CAPTION:Table showing locally available aliments in Mudzi District. In Care Groups mothers learn to prepare diversified and nutritious food using ingredients that remain available locally during the drought period – shown above are pumpkin leaves, baobab, eggs, milk, peanut butter and small dried fish.
CAPTION:Mothers belonging to a Care Group in Mudzi District are preparing a nutrient-dense porridge with locally available food to give to their young children to prevent malnutrition. Every week the mothers meet and discuss how to take care of their children, and ensure they remain healthy during the drought period their community is faced with. Through Care Groups the Ministry of Health and Child Care, UNICEF and partners distribute multiple micronutrient powders to add to children’s porridge and provide messages and counselling on good nutrition practices and behavior for caregivers of children younger than five years. Moreover, Care Groups teach mothers how to measure the mid-upper arm circumference (MUAC) of their children to screen them at home for early identification, referral and quality treatment of children with malnutrition.
UNICEF and its partners are preventing malnutrition among children and providing children suffering from malnutrition with high-quality treatment services. The case fatality rate for untreated severe malnutrition in children is more than 20%.
Any malnutrition increases the risk of death from common childhood illnesses such as respiratory infections and diarrhoea.
It is therefore crucial, especially in a drought year, to improve prevention of malnutrition and to ensure sufficient life-saving treatment services are in place for every child that needs them.
The programmes, developed by UNICEF, the Government of Zimbabwe and partners to prevent and treat malnutrition among children in districts affected by the El Nino-induced drought, are supported by United Nations Central Emergency Response Fund (CERF), the Health Resilience Fund, funded by the European Union, the Governments of Ireland and the United Kingdom and Gavi, the Vaccine Alliance, and internal UNICEF funds.
‘It’s a turnaround.’ A rural hospital credits village health workers and community influencers for transformation in uptake of services
Umguza, Zimbabwe – In a tiny office at Mbembesi rural health facility in Matabeleland North’s Umguza district, Thembinkosi Sibanda, a midwife, took stock of the numbers in the facility’s birth register. A contented smile followed.
Seven deliveries from the hospital’s maternity wing for the month. Only a single home delivery.
These are numbers she would hardly have imagined two years ago.
“We would usually record one or two deliveries here but most pregnant women would deliver in unsafe conditions at home,” said Sibanda, whose facility, surrounded by hard-to-reach rural and resettlement areas, now records between eight and ten births a month.
“It’s a turnaround,” she marveled, and, as if speaking to herself, added, “Job well done.”
Yet, Sibanda refused to take responsibility for the change.
“They are the real heroes, the credit goes to them,” she said, pointing to a group of village health workers (VHWs), local traditional and religious leaders and young people sitting in a shed for an advocacy meeting.
VHWs have forged a transformative partnership with community influencers to increase demand for, and access to primary healthcare services as well as engender improved water, sanitation and hygiene practices.
As part of interventions to strengthen primary health care services such as immunization, HIV services, non-communicable disease screening and treatment and health education, over 400 VHWs in 11 districts across several provinces recently underwent refresher training on how to intensify demand for services management and treatment of minor ailments at household level.
One of the results of those sessions, conducted by the Health and Child Care ministry in partnership with UNICEF and with funding from Gavi, the Vaccine Alliance, with funds from the Government of France, is the increased active participation of influential, authoritative, and trusted members of the community in amplifying the work of VHWs.
Authorities held community advocacy meetings with 1,500 key influencers who are trusted members of the community and included VHWs, interfaith and traditional leaders as well as young people such as peer educators to boost demand for COVID-19 vaccination, HPV vaccination, Vitamin A Supplementation and other vaccines amid successive outbreaks of measles, polio and cholera.
The meetings, done at ward and village level in all the 11 districts involved in the project, also discussed issues like demand for neonatal and postnatal care, HIV testing and treatment, COVID-19 self-testing, adolescent health services and how to intensify awareness campaigns.
Village health workers regularly attend refresher training sessions and cascade the information to community influencers who have become key partners in mobilisation and amplifying awareness campaigns
This kind of strengthening of primary health care support has contributed to increased referrals for vaccine hesitant groups and other children facing multiple deprivations.
The VHWs embarked on a journey to update their integrated village registers to record and account for every child in their respective communities and geo coding using ODK on their smartphones.
Out of the 3,879 zero children identified in 2023 in Umguza District, 3,685 – representing 95% – were successfully followed up and vaccinated.
Out of the 9,165 zero dose children identified in 2022 in the urban areas of Harare, Bulawayo, and Chitungwiza, 8,706, representing 95%, were successfully tracked and vaccinated.
The VHWs also recorded 24,424 under immunised children, with the majority referred or accompanied for vaccination.
Health authorities say they are roping in community influencers into some of their regular programmes to sustain the successes.
“Nowadays we also invite the influencers to the monthly meetings that we ordinarily have with Village Health Workers. They have become dependable partners for village health workers in mobilisation and awareness campaigns,” said Sibanda, the midwife at Mbembesi health facility.
Faith leaders have become key pillars in intensifying awareness and uptake of vaccines and other modern medicines among denominations whose doctrines undermine health seeking behaviours.
Traditional leaders such as village heads in the highly patriarchal community are now treating Village Health Workers, who are mostly female, as part of their inner circle.
Sheila Ncube is one of the 19 VHWs providing a link between Mbembesi hospital and people in hard-to-reach communities that are part of the facility’s catchment population of over 8,000 people scattered across the vast district.
With settlements opening up in the area, she needs her village head to point her to new inhabitants, who often lack basic water, sanitation and hygiene infrastructure and are also unfamiliar with health services offered in the area.
“The village head is the one who carries the word when I want people to gather for awareness sessions at a central point or when I am mobilising for campaigns such as vaccination. He is the one who helps me identify pregnant women in the village, he is my eyes and ears,” said the 70 year-old.
One of the village heads at the advocacy meeting, Lucky Sibanda, thinks the compliments belong to the VHWs, whom he describes as his mentors. Sibanda said he was previously indifferent to the services of Village Health Workers – until COVID-19 struck.
“They saved my community,” he said, referring to the VHWs.
“They educated people on prevention and treatment and many people ended up overcoming their fear of vaccines.”
When his local Village Health Worker approached him for help to mobilise for measles, polio, cholera vaccines following the outbreaks, Sibanda gladly obliged.
“The Village Health Worker is now my chief whip. She is always by my side when I hold functions. I have made it a rule that no gathering proceeds before she speaks about health,” said Sibanda. He reckons he is also turning into a campaigner, thanks to his increased interactions with VHWs and health workers.
Ongoing mentorship and coaching that has reached2,200 health workers and Village Health Workerson issues such as integrated service delivery, data collection, consolidation, analysis and reporting also cascades to community members such as traditional leaders, turning them into cadres.
“She teaches me whatever she would have learned from the workshops she attends. She has equipped me with information so much that nothing escapes me anymore, HIV treatment defaulters, sanitation and hygiene red flags, underweight children and pregnant mothers. I alert her as soon as I notice something amiss,” he said.
Heavy with pregnancy, 28-year-old Polite Ndlovu is one of those grateful for the intervention after being nudged by her village head and Village Health Worker to register her pregnancy at the hospital.
Pregnant women such as Polite Ndlovu are increasingly accessing quality neonatal and postnatal care at health facilities due to awareness spread by Village Health Workers and community influencers
“I planned to go but I was procrastinating but they warned me and other pregnant women in the village about the dangers,” she said.
“I went to the hospital the following day,” added Ndlovu on the grounds of Mbembesi hospital, where she had gone for a routine check-up.









































Recent Comments