Kadoma – During an active cholera outbreak, compiling and reporting high quality data on suspected cases – such as age, sex, location, symptoms onset, laboratory test results and treatment response – is crucial. This provides decision-makers with timely and accurate information to guide the cholera response.
To enhance reporting systems and cholera surveillance in Zimbabwe, the World Health Organization supported the Ministry of Health and Child Care (MoHCC) to conduct a data harmonization workshop in Kadoma.
The workshop aimed to address data quality gaps and update the missing cholera data across all provinces, including essential information like the effective utilisation of partner-donated resources such as cholera testing kits.
The WHO Data Harmonisation guidelines, which delineate surveillance data monitoring processes, were instrumental technical resources utilised by WHO to steer the data harmonization exercise.
Previously, data reported on cholera cases had missing information on laboratory tests conducted by healthcare workers across the country.
This shortfall undermined accountability and failed to accurately reflect the dedicated efforts of healthcare staff.
“We were putting in the hard work, but the data wasn’t reflecting that,” says Janet Jonga, manager for epidemiology and disease control at MOHCC.
“Now, we can showcase the impact of our efforts and this improved data will be instrumental in securing the resources needed to respond to outbreaks swiftly and save lives.”
Mr Jonathan Yadini, district health information officer for Hwange District commended the exercise and noted, “Previously, data from Laboratory and Surveillance was being reported separately in parallel data flow streams, leading to discrepancies in the data. This harmonisation exercise has promoted collaboration to ensure that cholera data is now accurately and comprehensively tracked through the health information database, enhancing epidemic monitoring.”
The harmonisation exercise was made possible with WHO support and enhanced data collection, with the line list completion rates soared from 70% to 95%, providing a much clearer picture of cholera transmission across the country.
Updating of laboratory data offered a comprehensive view of utilized resources, promoting better allocation.
The newly introduced district-level epidemiological curves with the up-to-date data helped to pinpoint areas experiencing challenges and enabled a more targeted community response.
Funding for this activity came from the UN Central Emergency Response Fund (CERF), and the Health Resilience Fund, (HRF supported by EU, GAVI, UK and Ireland).
WHO’s efforts have been focused but not limited to providing enabling factors to ensure early detection through equipping surveillance officers with skills for and enhanced testing of suspected cholera cases through provision of testing kits.
HO is also providing funding to ensure that data collected is transmitted daily and reflected in the situational reports of the MoHCC to promote timely information dissemination and action.
Supportive supervision visits are being undertaken periodically providing on the job mentorship.
The country now has a unified database of cases and deaths by district for the first time, enabling quick identification of areas of interventions.
This has promoted data driven decisions and interventions.
“Following this support, the MOHCC SITREP now features district level analyses thereby highlighting the situation in hotspot districts for attention,” said Mr Trevor Muchabaiwa, data manager at WHO Zimbabwe.
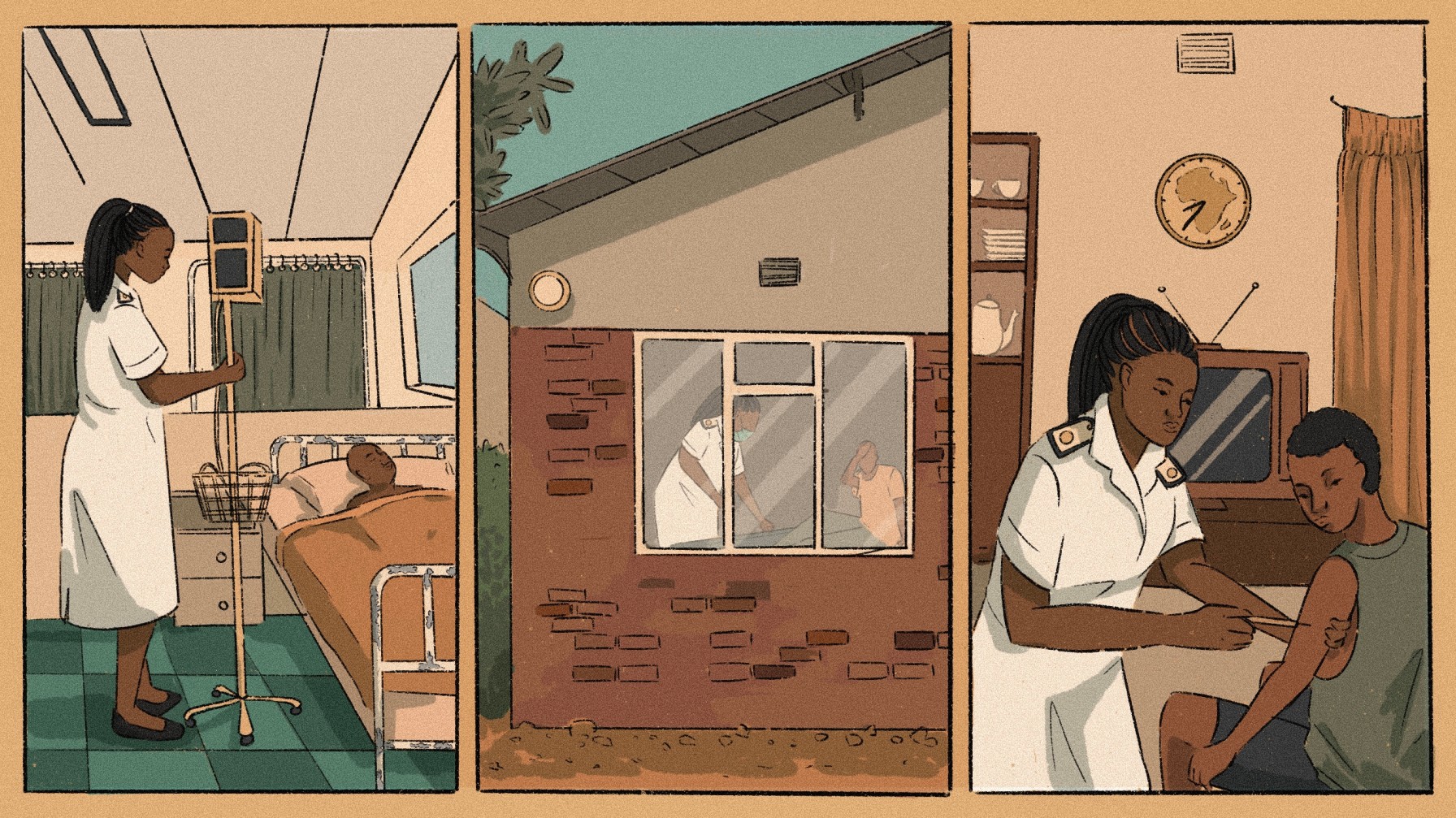
Those who remain must navigate a crumbling health care system — and the moral, physical and mental costs that come with it.
HARARE, ZIMBABWE — At five months pregnant with her second child, Vimbai started bleeding. She suspected a miscarriage and rushed to a public clinic for help. The attending midwife didn’t examine her, says Vimbai, who chose to use her middle name for fear of stigma.
“The only thing they did was [give] me cotton wool.”
To Vimbai’s shock, the midwife wrote “attempted abortion” on her consultation card and referred her to the nearest public hospital about 20 kilometers away (nearly 12.5 miles). But Vimbai was in too much pain to make it all the way. “I thought I was going to die.”
A friend recommended a nearby clinic operating illegally in someone’s home. “I had a conviction that this was the only immediate option,” she says.
Although the bed was uncomfortable, the home clinic was well equipped. There was a drip stand, boxes with cannulas, drugs and medical supplies stored in a tiny spare bedroom. The setup surprised Vimbai.
There were other patients too. Their murmurs seeped through the walls. Somewhere, a child coughed. Vimbai also noticed something else. She knew the nurse who operated the backyard clinic. He worked as a midwife at the public clinic where she had been first treated after the bleeding incident. To Vimbai, this meant he was qualified. It reassured her a little.
They confirmed she was having a miscarriage, put her on intravenous therapy along with some injections and he cleaned her womb, she says. Overall, the experience was friendlier, and the midwife followed up afterward.
“The hideout clinics are saving a lot of people in the communities [where] we live,” she adds.
Zimbabwe’s health care system has been crumbling under the strain of years of economic and political instability, which started in the late 1990s. Health worker salaries have not been spared by inflation and currency challenges.
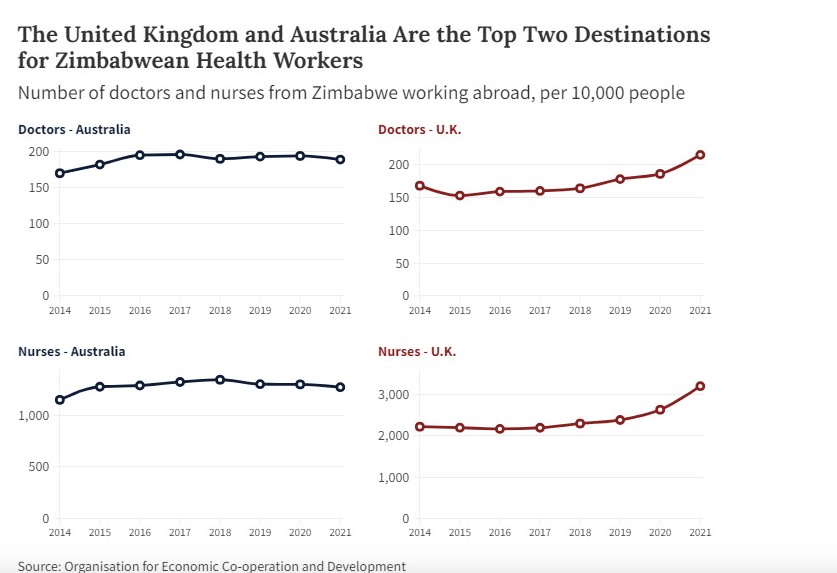
As a result, many professionals have migrated to seek better opportunities abroad. In 2019, the United Kingdom’s National Health Service employed 4,049 Zimbabwean health care professionals, including doctors, nurses and clinical support staff, making Zimbabwe the second-largest African contributor to its workforce after Nigeria, according to a statement provided to Global Press Journal by Zimbabwe’s Health Service Commission spokesperson, Tryfine Rachel Dzvukutu.
But not everyone leaves.
In late 2022, the country had 1,724 doctors and 17,245 nurses, Dzvukutu says, serving a population of over 15 million.
These doctors and nurses grapple with various challenges, among them poor salaries and high workloads. To navigate this, some take part-time jobs in other health centers while others operate illegal clinics such as the one Vimbai visited.
“Sometimes we resort to these hideout clinics not because we want to but because of the service we get at the public facilities,” Vimbai says, her voice tinged with discontent.
A MORAL DILEMMA
Gladys, who has been a health worker for 20 years and asked to use only her first name for fear of retribution, says that sometimes she offers services to people in her community outside of work, especially those who might need minor assistance, such as dressing wounds.
“I do charge for rendering that service,” she says. The cost ranges from 10 United States dollars or more per week, depending on what patients can afford.
In comparison, the clinic where she works charges 1 dollar a day for minor services such as wound dressing. But Gladys says her fees are typically lower than the overall costs a patient would incur, including transportation. Other times, she says she doesn’t charge if she sees that the person cannot afford to pay.
There has been an increase in these practices, even though it is illegal, says Simbarashe James Tafirenyika, president of the Zimbabwe Municipalities Nurses and Allied Workers Union. It’s also unethical, since the workers offering these services don’t have sterile equipment or other necessities, which is risky, he adds.
The Health Professions Act prohibits health institutions from operating without registration. Doing so is an offense liable to a fine, imprisonment up to two years or both.
(Gamuchirai Masiyiwa/Global Press Journal)
Gladys, who asked to use only her first name for fear of retribution, reviews her notes in a public clinic in Harare, Zimbabwe. To supplement her income, she occasionally provides services at patients’ homes.
Gladys doesn’t think she is bending the rules or posing any additional risks to patients; if they visit the clinic, she is still the same person who will assist them, she says.
However, she says those who operate more robust backyard clinics put people at high risk due to a lack of sterilised equipment. It is a criminal offense, she says, given the potentially fatal consequences, such as bleeding to death following an abortion.
Rueben Akili is a program officer with the Combined Harare Residents Association, an organization that advocates for the rights of residents. He confirms health care workers are operating illegal clinics in various high-density suburbs of Harare.
“It is an issue which we have noticed for the past five years due to the continuous deterioration of health service provision. They offer a range of services such as maternal health care provision, treating of sexually related diseases and to some extent general health care,” he says. He sees it as a worrying trend as it puts people’s lives in danger.
In a written response to Global Press Journal, Stanley Gama, the head of corporate communications for Harare City Council, says the council isn’t aware of illegal clinics but will carry out investigations and enforce the law. He adds that health workers, like every citizen in Zimbabwe, haven’t been spared by the challenges of the struggling economy.
Gladys says her salary at the public clinic where she works is low. In March, the government paid her ZWL$6 million (about US$195). (At the time Global Press Journal interviewed sources for this article, the Zimbabwean dollar was still the standard currency in Zimbabwe. The country has since transitioned to a new currency, called Zimbabwe Gold.)
Gladys also receives an allowance of US$112. The total amount she receives varies each month depending on the exchange rate.
To make ends meet, Gladys takes extra shifts or works as a substitute nurse at private institutions. She prefers shifts at private institutions.
The government clinic pays her US$4 for a full day of work, from 7am to 7pm, and converts the payment to local currency at the prevailing exchange rate.
The government also taxes this overtime pay. But the private health facilities pay her more money for fewer hours, at 20 US dollars for a day that ends at 4:30 p.m.
While extra work means more money, Gladys is always exhausted. She ends up working about 53 hours per week, well above the recommended 45 hours for health care workers.
“The body needs to rest. When you get home, all you want to do is sleep — you can’t do things that you would normally do like cooking, assisting your child with homework. We are overwhelmed,” says the mother of two. Her social life suffers too.
She knows colleagues who have quit the public clinic to work in private institutions and others who have immigrated abroad. Around 2017 and 2018, the public clinic had 22 midwives, she says. Now, it has 14.
She considered leaving Zimbabwe for better opportunities abroad, but when she wanted to start the process, the government stopped issuing certificates of good standing.
Without one, she would only be able to work as a care worker, which pays less than a professional nurse.
(Gamuchirai Masiyiwa/Global Press Journal)
As Zimbabwe’s health care crisis worsens with a mass migration of health care workers in search of better opportunities and low pay for those who remain, Gladys occasionally takes on extra shifts at her workplace or in private clinics.
The solution for Gladys is for the government to employ more workers and offer better pay.
Although health care workers left behind like Gladys are finding solutions — sometimes illegal — to navigate the challenges of a crumbling health care system, these arrangements are unsustainable, says Tafirenyika, the union president.
“What they are doing is bad and we do not recommend it at all, but they are looking for survival skills,” he says. He blames the local councils, which employ public health workers. The solution, he says, is to ensure an adequate health care workforce and offer them good pay.
Gama says the Harare City Council has been recruiting more health workers. He did not provide any figures.
Enock Dongo, president of the Zimbabwe Nurses Association, agrees Zimbabwe’s health workers are overwhelmed. The union is pushing the government to improve health workers’ pay and welfare, he says.
“It’s not only money that can solve the issues we are facing, but there are also many non-monetary benefits that they can provide like housing, land, farms, among others,” he says.
Although some health workers operate illegal clinics or take extra shifts to sustain their livelihood, others take up side gigs. Moyo, who prefers to use his clan totem for fear of retribution, is a nurse at a public hospital in Harare. He says his low pay gives him sleepless nights.
It is so low that he couldn’t add his fourth child to his medical insurance.
“I was told that my income was too low to have another dependent added on my insurance. I can’t even afford health care for my child,” he says.
In February, his salary inclusive of allowances was ZWL$3,6 million (US163 ) plus a foreign currency component of US$270.
According to the latest Zimbabwe Statistical Agency report on poverty, the minimum monthly income needed in March for one person stood at ZWL$916 255,50 (US$41,54). A family of six requires about US249 for food and non-food items to be above the poverty line.
Like Gladys, Moyo tried taking extra shifts at private clinics. He says lately they have been hard to come by. “Because of the economic situation in our country, the private health institutions are not getting as many clients as they used to,” he says.
In 2023, he registered a consulting agency to assist students with their applications to private nursing schools in Zambia.
“If I enrol 10 students, I get 20% commission. But because my company is fairly new, last year I managed to enrol three students and I was paid US$200,” he says.
Despite the challenges, Moyo still wants to advance in his career.
“I recently completed my bachelor’s degree in nursing science, majoring in training, because I have a passion to teach. And if conditions of service improve, I intend to work in a nursing school locally,” he says.
Although he could have relocated, he had someone close to him who was not well and he chose to stay. Home is best, he says. But those who leave are simply forced by circumstances.
Like most African countries, non-communicable (NCDs) diseases, including diabetes, is increasing in Zimbabwe. And children are increasingly among the cases that go undetected or treatment until severe symptoms emerge.
HARARE, Zimbabwe – Ten-year-old Tadisa Sayi already contends with diabetes and when his blood sugar levels spike his mother, Naume Shereketo, endures the mood swings induced by his condition.
Three years ago, Shereketo, a single mother of two, discovered the root cause of her son’s misery during a severe bout of illness.
“It was in 2021. He was weak and vomiting. When I went to the hospital with him, doctors told me he was diabetic,” Shereketo told Health Policy Watch.
“He always says: “Mama, I’m weak’, and some other time he is harsh,” said Shereketo.
Shereketo, a vegetable vendor on the streets of Harare, faces ballooning costs to attend to her son’s special dietary needs.
She struggles to provide the specific foods required for her son’s health. For Sayi, a grade four learner, fruit, vegetables, milk and high-fibre foods, have become a regular but costly part of his diet, costing his mother between US$60 and US$80 monthly.
Shereketo is puzzled about her son’s diabetes. No one else is diabetic in her family or the boy’s paternal side.
Dr Life Zambezi, the boy’s doctor, confirmed that Sayi had Type 1 diabetes, and said that this can be challenging to manage in young children due to limited support at the community level as well as the difficulty of maintaining strict insulin routines.
Type 1 diabetes, which causes glucose (sugar) in one’s blood to become too high, happens when a person’s body cannot produce a hormone called insulin that controls blood glucose.
Changes in diet also cause rise in Type 2 diabetes
While Type 1 diabetes is generally the result of a genetic condition, children also are being increasingly affected by Type 2 diabetes, as a result of changing diets and lifestyles, according to the UN children’s agency, UNICEF.
Type 2 diabetes typically develops as a result of sedentary lifestyles, obesity and unhealthy eating habits, Zambezi notes.
While it’s on the rise in most African countries, and usually associated with adults, he’s seeing more such cases among children.
“Of late, children are also getting Type 2 diabetes, mainly caused by the changes in lifestyle. There is a rise in poor eating habits among children. In most cases, they eat processed and unhealthy food leading to childhood obesity and eventually type 2 diabetes,” said Zambezi.
But diabetic children like Sayi are too often only diagnosed only when they have developed a severe crisis, such as a diabetic coma.
“NCDs in children result from a combination of genetic, environmental and behavioural factors,” then Health and Child Care deputy minister Dr John Mangwiro explained at the launch.
“When a young child is diagnosed with a non-communicable disease, this implies long-term treatment.”
CAPTION:Dr Life Zambezi says that the high cost of insulin has made life miserable for people with diabetes, many of who cannot afford the life-saving medication
Diabetes incidence in Zimbabwe soaring – although data remains spotty
Approximately 537 million people worldwide are living with diabetes, according to the according to the International Diabetes Federation (IDF), an umbrella organisation of over 240 national diabetes associations in 160 countries and territories globally.
That includes 422 million people worldwide suffer from type 2 diabetes, the majority living in low- and middle-income countries, according to WHO, of the disease that kills 1.5 million people every year.
That includes approximately 106,400 adults in Zimbabwe living with diabetes Type 1 and 2, a prevalence of 1.5% in the adult population of about 7.1 million, according to the International Diabetes Federation (IDF), an umbrella organisation of national diabetes associations in 160 countries and territories.
However, IDF’s local member, the Zimbabwe Diabetic Association, says that’s a woeful underestimate. It estimates that as many as 10 out of every 100 people in Zimbabwe’s population of 17 million had diabetes, including children, as of 2017. But many cases go undiagnosed until the child or adult in question becomes seriously ill.
A 2014 meta-analysis also suggests diabetes incidence has grown exponentially.
Prior to 1980, the prevalence of diabetes in Zimbabwe was just 0.44 %, while after 1980 the prevalence was 5.7 %, according to that systematic review.
As of 2016, Zimbabwe had the third highest estimated per-person cost of diabetes care in sub-Saharan Africa.
Insulin’s exorbitant prices also cause many to miss out on essential medication, exacerbating their condition and long-term health risks, Zambezi said.
Treatment at primary health care level is spotty
Treatment in primary health clinics remains spotty, the studies also suggests.
One small study comparing treatment in primary versus hospital facilities in Harare, the capital city, found that more patients treated at hospital outpatient clinics and received some form of diabetes self-management education (DSME), and had higher levels of diabetes knowledge, as compared to those treated in primary care facilities.
At the same time, people who had consulted a dietician had the best levels of diabetes knowledge and self-care routines.
“Dietitian-led interventions significantly improved both knowledge and practices, highlighting a need to scale up dietetic intervention, particularly in primary clinics where limited interventions occur,” concluded the July 2019 study led by a researchers at the University of Cape Town and the University of Zimbabwe’s Department of Community Medicine.
“Though improvements have been made in self-management therapies, there seems to be a high prevalence of hospital admissions with relapse of symptoms in Zimbabwe. Relapse in diabetes predicts poor prognosis,” concluded another, 2021 study, led by the University of Zimbabwe’s Department of Nutrition.
Recognizing those gaps, UNICEF in 2022 launched an initiative in five countries including Zimbabwe, to focus on NCD prevention, detection, treatment and support, particularly in children and young adults.
As part of the grant, funded by the pharma firm, Eli Lilly, Zimbabwe’s Ministry of Health received US$2.5 million to educate community health workers and increase support and understanding of various NCDs including diabetes in children.
Late detection and poor management results in adult complications
CAPTION:Diagnosed with diabetes 20 years ago, 30-year-old Tariro Chiripanyanga is now contending with end-stage kidney disease as a result of poor management of her diabetes
But until earlier detection and prompt treatment become more of the norm, many children will continue end up with severe complications in early adulthood, Zambezi observed.
One such case is Tariro Chiripanyanga.
The youngest of four siblings, Chiripanyanga was diagnosed with Type 1 diabetes at the age of 10.
Today Chiripanyanga is now facing end-stage kidney disease, although she is only 30 years old.
“I was still too young to understand what it meant or how it would affect my life, but that’s when my life changed forever,” Chiripanyanga told Health Policy Watch.
Apart from living with diabetes since childhood, Chiripanyanga was diagnosed with kidney disease six years ago.
She needs US$30,000 for a kidney transplant, a financial burden neither she nor her family can bear.
Chiripanyanga’s diabetes has already led to partial blindness, forcing her to drop out of university.
“My life depends on peritoneal dialysis which costs US$1,750 monthly,” Chiripanyanga said.
“I depend on dialysis until I can get money for a transplant which costs an estimated US$30,000 in India.”
“We do business differently.” A revived health club has transformed into a savings club, using a business model to promote sanitation, hygiene and nutrition.
GUTU, Zimbabwe – After an opening prayer, members of the Jekesa Kuface health club in Masvingo Province’s Gutu District launched into one of their signature songs with the lyrics: “Cholera, we will not tire until we defeat you.”
Then it was time for life-saving business.
“Is everyone paid up? Because we will all suffer if we don’t keep up with our payments, cholera is no joke people, it kills,” the club’s chairman, Johnson Rwodzi, said. He went through a book with a list of names, payment details and progress on construction of toilets and other sanitation and hygiene infrastructure.
Jekesa Kuface, which translates to “brighten up the face”, is more than just a community health club is one of several health clubs recently revived with the help of the Ministry of Health and Child Care, UNICEF and partners under interventions spearheaded under the United Nations United Nations Central Emergency Response Fund (CERF) in response to Zimbabwe’s cholera outbreak.
Jekesa Kuface health club
For members, Jekesa Kuface, initially formed in 2017 before faltering due to lethargy, has become more than just a health club to fight cholera.
“We do business differently. We are an empowerment forum, a way of life. We are integrating awareness with practical interventions in health and people’s general economic welfare,” said Rwodzi.
Since its revival in January, Jekesa Kuface has transformed itself into a savings club that is using sheer business acumen to ensure that apart from being a vehicle for health education, it empowers members with resources to construct hygiene infrastructure such as toilets in an area with a history of open defecation.
In addition, it is building the resilience of members to cope with food insecurity that affects the nutrition of children and ensuring people reap some money to pay for essentials such as their children’s education.
The concept is simple, yet effective.
Each member contributes US$1 each time the club meets.
The money is pooled into a savings pot and then invested in the form of loans to members and other community members at 20% interest.
The profits go towards assisting each member to build a toilet at their homestead.
CAPTION:A member of Kujeka Kuface Health Club records details of payments and activities. The health club has transformed itself into a savings club and uses a cooperative business model to respond to health challenges.
“That way, we ensure that even those who ordinarily would not afford to construct a toilet are able to because the money is available to buy cement and other items. Put simply, we are building toilets for each other,” said Rwodzi.
He explained: “A member digs their own hole, but we help them if they are elderly. They source mesh wire for the slab and buy two bags of cement. The club chips in with three bags of cement and also helps with the labour. Once we are done, we move to the next member.”
The target is for each member’s homestead to boast of a toilet by the end of the year.
Influencing community behaviour
On some days, club members conduct clean-up exercises in the village, hoping to change the attitudes of fellow community members.
At gatherings such as funerals, weddings and community meetings, they innovate with drama, song, dance and poetry performances to capture the attention of people and attract some who are still resistant to their messages, especially men.
Only two members of the club are men, a composition that highlights the challenges of convincing men to participate in activities they traditionally view as reserved for girls and women.
CAPTION:Health clubs and village health workers are driving social, and behaviour change campaigns in Gutu district in response to cholera, malnutrition and food security challenges.
Ten health clubs have been revived or newly established since the CERF intervention kicked in at the beginning of 2024.
Realising the need to quickly act to prevent disastrous loss of lives and livelihoods during underfunded humanitarian emergencies, the UN General Assembly established CERF as a global emergency response fund in 2006.
In Zimbabwe, CERF allowed UNICEF and partners to intervene in five districts in Masvingo, Manicaland, and Matabeleland South provinces to prevent malnutrition and disease outbreak through the provision of access to safe water, sanitation and hygiene.
Toilets
Apart from provision of water infrastructure, the intervention has an emphasis on social and behaviour change underpinned by the participation of affected communities to improve awareness of safe hygiene and sanitation practices – a key factor in the prevention of waterborne diseases such as cholera.
At the core is the empowerment of village health workers (VHWs) through refresher courses and other incentives and the resuscitation or establishment of community health clubs such as Jekesa Kuface to spearhead the spread of information on critical lifesaving water, sanitation and hygiene practices.
These include construction of toilets, waste management pits, water treatment and a healthy diet for both adults and children.
In Gutu’s Rwodzi village, such ideals were seen as too lofty only a few months ago in a community where many people were either too poor or lacked information to prioritise their health and that of their children.
But the revival of the health club has changed the tide.
Rejoice Moyo is one of those whose life has changed for the better. She recalls what she describes as the “ignorant days.”
Before joining the health club, the 40-year-old mother of seven hardly regarded a toilet as a priority need.
When her infant children asked to poop, she would take them to the back of a kitchen hut.
For her and other older members of the family, nearby bushes provided enough cover to defecate away from prying eyes.
“It didn’t even occur to me that what I was doing was hazardous,” she said, clad in a blue t-shirt inscribed with anti-cholera messages.
“Our club and the Village Health Worker opened my eyes. I now have a toilet at home, I have dug pits for waste disposal and I make sure my environment is always clean,” she said.
That’s not all. She no longer fears for her children getting malnourished because the health club has introduced a system where members help each with manual labour and knowledge to establish nutrition gardens that are providing both food and income, she said.
“From this meeting I am going to sell my vegetables. My husband is unemployed so I have become the breadwinner,” said Moyo.
Authorities say they are seeing some change.
“There is a great difference,” said Absolom Madzana, the Gutu district principal environmental health technician.
“Open defecation is becoming a thing of the past because Village Health Workers and health clubs have become key drivers of the construction of toilets. We had ten toilets built within two months, which is within our target of five toilets per month,” he said, adding that six community members have been trained as builders “and have been busy at work.”
The rate of people reporting to Chimombe Rural Hospital, where Madzana is based, with diarrhoeal diseases have dropped from an average of 20 cases per month to six, while cholera cases have not been reported in recent weeks following the UNICEF funded CERF intervention, said Madzana.
But that is no reason for complacency, with village health workers knocking door-to-door and addressing community meetings for awareness and surveillance.
“I have told them to always be on alert to prevent an outbreak. It takes time to stop an outbreak and it also takes a lot of resources,” he said.
“Prevention is better than cure,” added Madzana, before addressing a meeting of Jekesa Kuface Health Club.
UNICEF’s cholera response is funded by multiple donors, including the Centres for Disease Control and Prevention; the European Civil Protection and Humanitarian Aid Operations; the Health Resilience Fund, a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; the Government of Japan; the UN Central Emergency Response Fund and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from United Parcel Service Foundation.
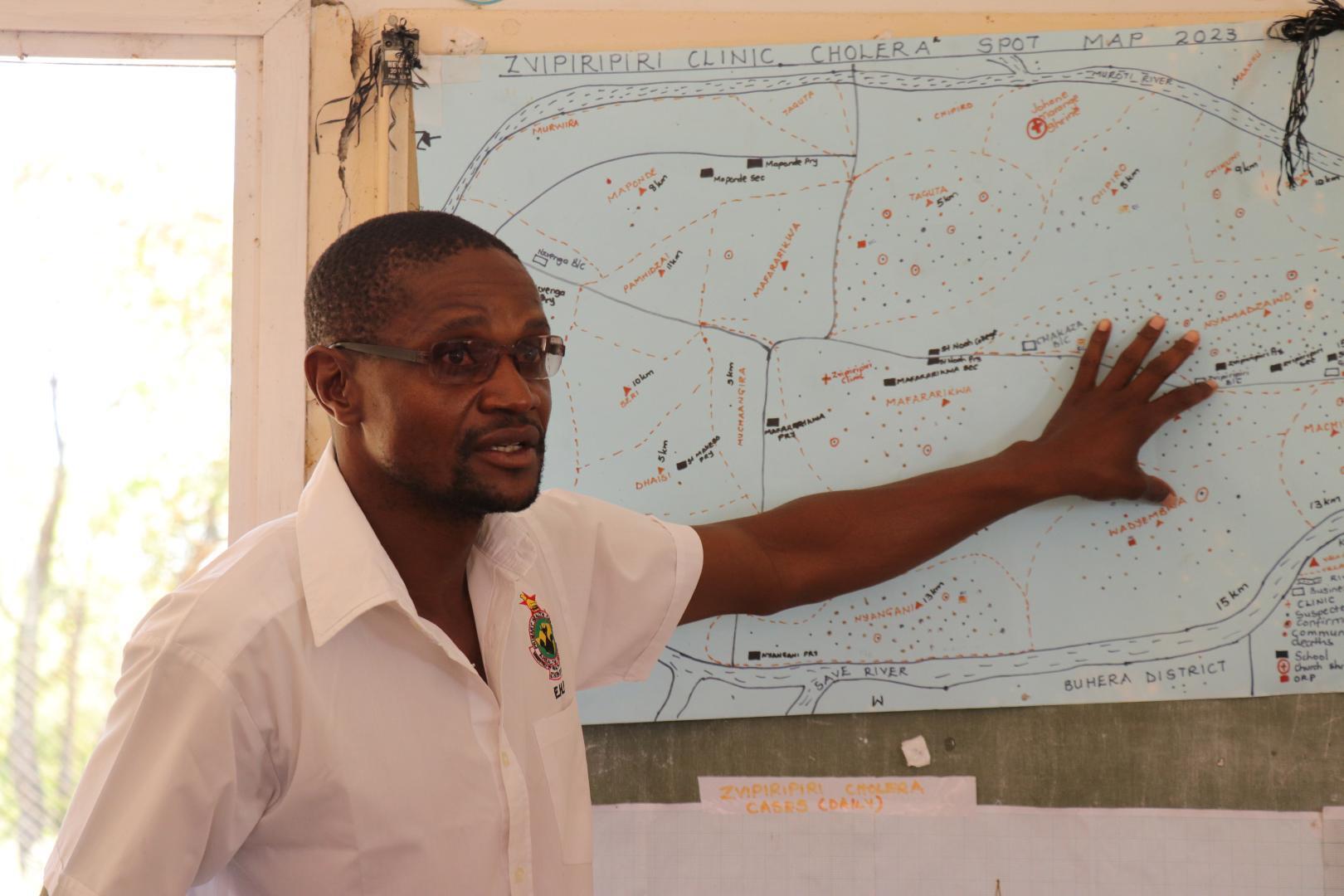
CAPTION:Zvipiripiri Rural Health Centre environmental health practitioner Lovemore Mudzingwa explaining the distribution of cholera cases
Mutare – The number of cholera cases in Zimbabwe is declining thanks to the expanded and decentralised cholera response activities undertaken by the Ministry of Health and Child Care (MoHCC), supported by WHO and other partners.
While current figures remain higher compared to the same period last year, this reduction is a welcome development, given the alarming surge between November 2023 and January this year.
At the peak of the outbreak in Manicaland province, Lovemore Mudzingwa, an environmental health practitioner (EHP) at Zvipiripiri Rural Health Centre, played a critical role.
He tirelessly responded to rumors in the community, providing essential information and disinfecting homes of suspected patients after assisting with their transportation to the clinic.
CAPTION: A CTC at Zvipiripiri
Driven by a commitment to making a difference, Lovemore works hard to ensure his community has accurate information on cholera and other diseases.
He actively identifies and addresses potential contamination sources, conducting regular inspections of water and food facilities to enforce hygiene standards.
“Our responsibility extends beyond responding to outbreaks,” says Lovemore.
“We strive to prevent them altogether. By educating communities on the importance of safe water, sanitation, and hygiene practices, we empower them to protect themselves and their families from cholera.”
Lovemore’s dedication saved lives.
In Mutorera Village, Zvipiripiri, his intervention helped 11 members of a single family survive cholera, with one succumbing to the disease.
One survivor, 21-year-old Clara Marime**, expresses her deep appreciation for Lovemore and the other health workers at Zvipiripiri.
Coming from a religious group that often avoids modern medicine, her experience was particularly challenging.
“I’m grateful to be alive,” she narrates.
“By the time I reached the clinic, I was completely disoriented. I only realized where I was a day later.”
While their efforts often go unnoticed, EHPs play a vital role in cholera outbreaks.
They manage funerals during outbreaks, coordinate emergency response efforts, and provide crucial support to affected communities.
CAPTION: A CTC at Zvipiripiri
From setting up cholera treatment centres to conducting contact tracing and disease surveillance, their expertise is vital for containing the spread of the disease and saving lives, not just from cholera.
Since February 12th, 2024, Zimbabwe has been grappling with a cholera outbreak.
As of 11 May 2024, a total of 33,914 suspected cholera cases have been reported nationwide, with 87 confirmed deaths, 623 suspected deaths, and 3,963 confirmed cases.
Manicaland province alone recorded 6,596 cases during the same period.
In Zvipiripiri, WHO leveraged funding from the Health Resilience Fund (HRF) to strengthen the cholera treatment center.
The facility was expanded from eight beds to twelve and provided essential medical supplies like rehydration fluids, antibiotics, and other cholera-specific treatment materials.
Additionally, WHO supported the installation of sanitation facilities like waste pits and emergency latrines to promote hygiene and prevent further transmission.
Triage points were also established to ensure an organized flow of patients and staff, minimizing infection risks.
Furthermore, in November 2023, WHO provided the province with essential supplies including medicines, personal protective equipment (PPE), information, education, and communication (IEC) materials, and cleaning and disinfection supplies to bolster response efforts.
In addition, WHO, with the support from HRF and Central Emergency Response Fund (UNCERF), spearheaded training programmes for EHPs, reaching over 60 individuals from all districts across the country.
These trainings focused on water quality monitoring, equipping EHPs with the knowledge and skills to effectively test and analyse water samples.
To further strengthen water quality surveillance in communities and especially in CTCs, WHO procured and distributed water quality kits and consumables.
Additionally, WHO provided training on food safety for 115 EHPs, empowering them with current food trends, standards, and knowledge on foodborne illnesses.
They gained valuable skills in preventing and controlling cholera and other diarrhoeal diseases, including vital measures to be implemented in communities and CTCs.
On the job mentorship to EHPs on infection prevention and control and community engagement activities in CTCs and communities in response to the cholera outbreak is still being provided.
“The significant decline in cholera cases in Zimbabwe is a testament to the collective efforts of the MoHCC, WHO, and other partners. However, our work is far from over. We must continue to support communities to strengthen prevention efforts to ensure a lasting impact on public health,” notes Dr Sally-Ann Ohene, WHO Zimbabwe cholera incident manager.
**Names changed to protect identity of the contributor.
A Zimbabwean health worker administers an HIV test
HARARE, Zimbabwe – Michelle and Michael Mutsvaki were infected with HIV at birth, but while their parents have shunned antiretroviral (ARV) medicine to treat their HIV, the siblings opted for treatment in their teens.
The siblings, now aged 22 and 24, learnt about their HIV status from their mother, but she assured them that their faith would protect them from succumbing to the disease.
However, faith did not save their father. Instead, they watched him die of HIV complications a decade ago despite the intervention of faith healers.
Meanwhile, their mother, a follower of the African indigenous Johane Masowe Church, still clings to her religious beliefs and concoctions instead of taking ARVs.
But after Michelle and Michael learnt about the importance of taking antiretroviral treatment from HIV/AIDS activists who visited their school in 2017, they made one of the most important decisions of their lives, opting to take ARV treatment despite their parents’ advice. Seven years on, they are doing well.
The siblings were both born at home without the assistance of nurses because their parents avoided clinics and hospitals due to their religious beliefs.
Labour and birth is a risky time for newborn babies born to mothers with HIV who are not on ARVs with suppressed viral loads as they can be exposed to the virus in bodily fluids.
But mother-to-child HIV transmission, also referred to as vertical transmission, is rare nowadays as pregnant women with HIV take ARVs to ensure that their viral load is undetectable before giving birth, meaning that the virus is untransmissible (referred to as U=U) . Newborns are also given ARVs at birth to prevent infection.
Unfortunately, being born at home without medical help, Michelle and Michael contracted HIV at birth.
Citizens embrace ARVs
Zimbabwe’s adult population has come to embrace HIV treatment. The Zimbabwe Population-based HIV Impact Assessment Survey conducted in 2020 revealed 86.8% of adults living with HIV knew their status, and of those who were aware that they were living with HIV, 97% were receiving antiretroviral treatment.
About 1.4 million people in Zimbabwe are living with HIV, and the health ministry says that some 1.2 million Zimbabweans are on ARVs.
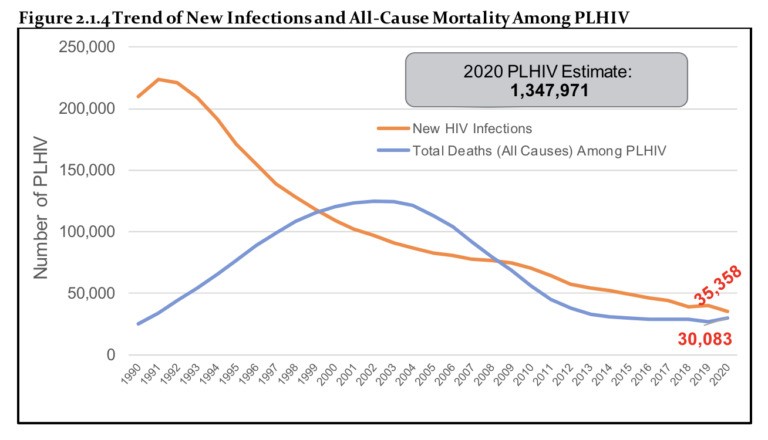
The huge uptake of ARVs has been the main reason for a 50% decline in the national HIV incidence over the past 10 years, according to a report from UN Development Programme (UNDP), which works with the health ministry and the Global Fund to prevent HIV.
HIV prevalence in adults (15-49 years) has fallen from its peak of 26.5% in 1997 to 11% in 2021. In 2022, the incidence rate of new infections was at 0.17%, and there was a decline in new HIV infections for all age groups.
Meanwhile, AIDS deaths have also plummeted over the past 20 years. In 2002, an estimated 130,000 people died of HIV-related complications whereas by 2021, the death toll was around 20,200, according to a UNICEF report.
People living with HIV wait to collect their share of free life-prolonging ARVs at Sally Mugabe Hospital in Harare
Treatment holdouts
Yet as the southern African nation registers success in combatting HIV/AIDS, other people living with the disease have remained adamant they will not take treatment.
Susan Mutsvaki, Michelle and Michael’s mother, has openly expressed contempt for ARV drugs, citing her faith as a barrier to taking modern medicines for any form of illness
Mutsvaki, aged 47, says she has lived with HIV for the past two decades without taking any treatment or ARVs. Instead, she firmly believes that a concoction of water and pebbles that she was instructed to drink by her bishop at her church a decade ago, has helped keep her safe while living with HIV.
Mutsvaki is a member of the Johane Masowe Church, which traditionally worships at open-air gatherings with all congregants donning white garments.
Mutsvaki operates a market stall at the Rezende Bus terminus in central Harare, where she sells fruit, vegetables, popcorn and cigarettes.
She keeps a white bag with her that contains a 750 ml bottle of water mixed with pebbles, which she sips from, as told by her religious leader whom she refers to as a “prophet”.
“I have not been sick at all from HIV. This bottle and the stones in it are my prayers from our prophet and I believe these are making wonders for me as you see how fit I look,” Mutsvaki said.
While Zimbabwe prides itself of achieving success in preventing HIV/AIDS, there are a few holdouts who have pulled in the opposite direction.
Hector Chinopa is one of these. When he contracted COVID-19 in 2020, he asked staff at the Wilkins Hospital in Harare for an HIV test, which came out positive.
But barely four years after surviving the coronavirus, 36-year-old Chinopa has been dodging antiretroviral drugs.
Like Mutsvaki, he reasons that he has not been ill since contracting COVID so he hasn’t felt a strong need to seek treatment.
“I’m not sick. Do I look sick when you look at me? No, I’m not sick,” Chinopa told Health Policy Watch.
Zimbawe’s death toll has plummeted since introducing ARVs
Teen sons may have died of HIV
Linet Gavi, 41, who tested HIV positive two years ago, also has not taken any treatment. But she is uncertain about whether her two teenage sons, who passed away in 2019, were living with HIV.
The boys, aged 15 and 18 at their deaths, suffered from severe headaches and coughing, and had bouts of diarrhoea, according to their mother. They vomited often and they both lost their hair and weight during the time of their illness.
At that stage, Gavi was in the dark about her HIV status. Since she was diagnosed, she wonders whether she might have passed the virus to them at birth.
But Gavi is resistant to taking ARVs because she claims she has witnessed friends and family becoming seriously ill after beginning ARV treatment.
“I don’t want to die by taking ARVs. I had relatives and friends who took ARVs after suffering from HIV, but they are no more today. I’m fine without treatment and I have not been sick. I just eat some crushed garlic to boost my immune system,” Gavi claimed.
Chinopa, Gavi and Mutsvaki all said they have not dared seeking treatment from government clinics after testing positive for HIV although the Zimbabwean government has been making urgent calls for all HIV patients to be placed on treatment.
Zimbabwe’s prevention of mother-to-child HIV transmission programme has been operational since 2002, transitioning from a pilot program in 1999 to a national initiative. Children born since then, such as Michelle and Michael, could have been spared HIV infection if their mothers consulted clinics and gave birth in health facilities.
International help
Between 2003 and 2022, the Global Fund has invested $1.8 billion in Zimbabwe’s HIV programme and recently approved a three-year HIV grant of (2024-2026) $437 million.
Despite a few people refusing ARVs to this day, Zimbabwe has made significant strides in prevention and treatment.
An official from Zimbabwe’s Health Ministry, who declined to be named, told Health Policy Watch, that ARVs were available for everyone who tested postive for HIV and were willing to take the treatment.
“Those people you say are refusing treatment are making their own decisions not to have the ARVs, but I can tell you the treatment is available for all who test positive for HIV,” said the government official, who was not authorised to speak to the press.
Although some Zimbabweans are resisting HIV treatment, late last year authorities announced that 95% of its HIV-positive population reached undetectable levels of the virus.
In November 2022, the Ministry of Health’s Dr Chiedza Mupanguri told a media briefing that 95% of Zimbabweans living with HIV had reached undetectable viral loads, meaning that the level of virus in their bodies is so small it cannot be transmitted to others.
This year, Zimbabwe became the first country in Africa, and the third in the world behind Australia and the US, to approve CAB-LA, a long-acting injectable medication that prevents HIV.
CAB-LA acts as a pre-exposure prophylaxis (PrEP) and is recommended by the World Health Organization (WHO) for those at high risk of contracting HIV.
While the country has pledged to target the entire population in its battle against HIV, individuals like Chinopa, Gavi, and Mutsvaki remain steadfast in their refusal to participate.
HIV/AIDS activists attribute the current deaths to those living with the disease for rejecting treatment due to myths suggesting that the drugs intended to help them actually hasten their demise.
“Many getting killed by AIDS these days are either defaulting on treatment or not on treatment at all,” Moris Mukundu, an AIDS activist in Harare, told Heath Policy Watch.
Zimbabwean innovators have built a chatbot connecting pharmaceutical drug vendors and registered health-service providers to customers. It is used via the WhatsApp messaging application.
Dubbed Cloomi, the WhatsApp chatbot has become very popular in Zimbabwe, a country where the health sector has been deteriorating for years.
It is common practice that public and private hospitals lack the required drugs and prescription. As such, citizens must find a pharmacy to buy pharmaceuticals.
On Cloomi, Zimbabweans at home and in the diaspora can check the availability and compare prices of services and products offered by pharmacies and medical laboratories in their chosen location.
“Talking to the bot like they are chatting to one of their friends, a user selects the category of providers they want, enters a city or area and the product or service he or she is looking for,” says the co-founder of Cloomi, Blessing Museki, a Zimbabwean software engineer based in the United Kingdom.
Cloomi was founded in 2022 after discovering how difficult it was to find the price and availability of essential medicine in Zimbabwe.
It prioritises the privacy of users by allowing anonymous identities.
“When attaching a prescription, we ask the user to obscure any personal details, which is pretty easy to do with WhatsApp,” says Museki.
According to Museki the application adopts other easy use features.
“You can specify what you are looking for in plain text form, like “paracetamol”, or attach a picture that is a prescription or product bottle or packaging.”
He says this request is then instantly sent to all the subscribed service providers that match the user search.
Using the same bot service providers can download and process customer requests.
Normally, users receive an availability confirmation or price quote within at least ten minutes.
The pharmacy can confirm if they have the product by providing information like price or asking the user for a prescription.
The user can also see the business’s physical address and location on a map.
Armstrong Manenji, a marketing and research officer at Greenwood Wholesalers and Pharmacies, says that the technology has been embraced mainly by people abroad.
“It is easy to use. People living abroad find it convenient because they can look for, order and pay for medicine for their relatives and ask them to collect at the pharmacy,” he says.
Pharmacies with online payment options are preferred by diaspora users.
Cloomi however has a limit. A service provider can only respond to requests within 24 hours. “You might be busy and need more time to respond,” says Manenji.
Service providers who fail to respond within that time end up losing potential clients.
Cloomi uses the WhatsApp platform, popular in Zimbabwe, as opposed to web browsers affected by slow connection and expensive internet data fees.
To date, more than 200 pharmacies and 10 medical laboratories across the country have come on board.
“Later on, we are going to include doctor booking via the chatbot,” Museki says.
Health Resilience Fund strengthens access to primary health care in the most remote places in Zimbabwe
In Matabeleland South Province, the Health Resilience Fund is changing access to primary health care services. We saw many happy faces during a recent media field mission to Gwanda, Umzingwane, and Bulilima Districts with the Ministry of Health and Child Care and the Health Resilience Fund Communication Officer. Local communities expressed gratitude for the strengthened healthcare delivery system, which makes basic essential healthcare services available to all, including those in the most remote areas of the Country.
The Health Resilience Fund is a coordinated effort by the Zimbabwean Government and development and technical partners supporting the Ministry of Health and Child Care in attaining Universal Health Coverage for the people of Zimbabwe.
The Fund is led by the Ministry of Health and Child Care and benefits from financial contributions from the European Union, the Governments of Ireland, the United Kingdom, Gavi, the Vaccine Alliance, and technical support from UNFPA, UNICEF, and the WHO.
The programmes supported by the Health Resilience Fund are implemented by the Ministry of Health and Child Care at national, provincial, district and community levels and by implementing partners.
The Health Resilience Fund is about bringing health care close to the people. In the Plumtree District Hospital, a student nurse aide consults a local patient to provide her with the most accurate health services.
The Health Resilience Fund supports the Plumtree District Hospital by training healthcare workers, providing clinical mentorship for doctor-nurse teams, and providing health supplies and medicines.
It functions as a referral hospital for the local health facilities in the area.
Through the support provided at the hospitals and health facilities at the national, provincial, district and local regional levels, the Health Resilience Fund aims to reduce maternal, neonatal and child mortality and teenage pregnancies and to strengthen health systems to tackle current and future health challenges.
The Health Resilience Fund focuses on women, neonates, children under 5, adolescents, youth, and vulnerable populations, including people with disabilities and marginalised populations.
Particular attention goes to the health of adolescent girls, as Zimbabwe faces high levels of early pregnancies.
The Adolescent Pregnancies in Zimbabwe, published recently by the Ministry of Health and Child Care and UNICEF with the support of UNFPA and UNESCO, indicates an adolescent pregnancy prevalence rate in Zimbabwe of 23.7 per cent.
At Plumtree District Hospital, 29 out of the 34 mothers seen at the maternity waiting home on the visit’s day were adolescents under 19.
The nurse in charge of one of the health facilities in Umzingwane District proudly showed her pharmacy.
Thanks to the support of the Health Resilience Fund, drug shortages have become rare in her facility. Accessing essential medicines is key to the Health Resilience Fund’s ultimate objective.
This accessibility contributes to ensuring Universal Health Coverage for all Zimbabweans, meaning everyone in Zimbabwe has access to a full range of quality health services without financial hardship.
Ensuring Universal Health Coverage implies health services are brought to the people, like here through an outreach activity in Matabeleland South.
To end preventable deaths in maternal, newborn and child health, interventions of the Health Resilience Fund emphasise increased availability, equity and access to essential reproductive maternal, new-born, child and adolescent health and nutrition services, including through promoting community participation and bringing health services as close as possible to the people’s everyday environment.
It took us more than two hours driving from Bulawayo, primarily over dirt roads, to reach one of the outreach activities set up by the District Health Office in a remote area of Gwanda District.
Various health interventions were offered to the local communities with the support of the Health Resilience Fund.
Interventions included routine vaccination, vitamin A supplementation and growth control for children, family planning, a wide range of outpatients’ department services, postnatal care (PNC), HIV testing, counselling and treatment, eye-testing, COVID 19 self-testing, visual inspection with acetic acid and camera (VIAC) to prevent cervical cancer in women aged 30-50 years old, and drugs distribution.
The outreach activities mobilised a large group of people across all age groups from the surrounding communities, most of whom do not have any other opportunity to access essential health services.
Village Health Workers are vital to linking people in need with health care services. They have the best understanding of the local communities.
They are crucial in mobilising mothers to bring their small children for preventive and curative health services to the local health facilities and outreach activities.
Village Health Workers have been instrumental in reducing the maternal mortality ratio from a peak of 960 in 2010 to 462 per 100,000 live births in 2019 and of the infant and under-five mortality rate from 67 and 94 in 2010 to 47 and 65 per 1,000 live births in 2019.
Hundreds of people have died of cholera this year in Zimbabwe, where the lack of adequate water and sanitation fuels an uncontrolled outbreak.
In Zimbabwe, water supply challenges, lack of access to sanitation and hygiene, and prolonged dry seasons caused by climate change have exacerbated a cholera outbreak that has killed hundreds of people this year.
The latest outbreak began in the town of Chegutu, about 60 miles south of the capital city, Harare, where the first patient with cholera was reported in February 2023. The number of cases increased throughout 2023, spreading to 10 provinces throughout the country. Cholera cases are still rising, with 35,000 recorded cases and 600 deaths in 2024 alone.
In addition to straining Zimbabwe’s health care systems, the outbreak has exposed vulnerabilities in water, sanitation, and hygiene infrastructure in both rural and urban areas. This has heightened the risk of transmission. The limited global supply of oral cholera vaccines has further complicated response efforts. Below, two experts with Doctors Without Borders/Médecins Sans Frontières (MSF) Southern Africa explain why a new approach is needed.
By Phillip Aruna, MSF regional operations team leader, and Mounia Amrani, MSF regional medical team leader Zimbabwe is grappling with the second-largest cholera outbreak in its history, with cases rapidly spreading across the country. It started on February 12, 2023, and to date, more than 600 people have died from cholera and over 35,000 have been infected. To save lives and prevent more people from falling sick, Zimbabwe has to invest in its water sanitation and hygiene infrastructure.
Cholera is a potentially deadly disease that is caused by bacteria that live in water. Access to clean water, proper sanitation infrastructure, and hygiene measures reduce the likelihood and severity of cholera outbreaks. Recurring outbreaks in Zimbabwe are a problem caused by old and degraded water and sewage systems in urban areas. Certain cities, such as Harare, have endured months without running water, with raw sewage becoming a common sight in the densely populated suburbs.
Rural communities are affected because they are resorting to drinking unsafe water from the surrounding rivers. The lack of substantial, adequate rain has compounded the situation both in urban and rural areas, with the water table depleting.
In Zimbabwe’s Buhera District, where MSF teams supported the Ministry of Health and Child Care in the fight against cholera for three months, villagers have had to drink river water, which they shared with wild and domestic animals. Boreholes have broken down, leaving them with no other options. Unsurprisingly, cholera did not spare Buhera.
MSF also intervened in Mbire District, about 120 miles north of Harare. In Mbire, our teams noticed there was 52 percent coverage for safe water sources, while 48 percent was from the river, and a paltry 37 percent latrine coverage. When people from Mbire work their gardens and fields along the river, they consume water from the river, which is unsafe. Without toilets in the fields, community members resorted to using bush toilets along the river.
“We bathe and drink water from the stream. There is no other source of water, and we are used to this. Recently, miners started complaining of diarrhea.” — Lasten, a miner Kamudonzvo in Shamva
Mining communities are also recording a high number of cholera cases. Miners access water from contaminated sources like dumped mining pits and nearby rivers, creating a breeding ground for cholera. This is the case in Shamva district, where MSF teams recently provided support. Open defecation and limited sanitation facilities further exacerbate the situation.
Villagers have had to drink river water, which they shared with wild and domestic animals. Boreholes have broken down, leaving them with no other option. Unsurprisingly, cholera did not spare Buhera.
Another population recording a high number of cases is a conservative religious community that objects to contemporary medication. They believe in using water for bathing, which sometimes contaminates water sources. Many cases are believed to have emanated from their gatherings.
The common element between all these communities is the lack of access to clean water and adequate sewage facilities. This problem urgently needs to be addressed to control the cholera outbreaks.
In theory, cholera vaccines could also help to control the disease. Unfortunately, there’s a global shortage of oral cholera vaccines today and Zimbabwe doesn’t have enough doses to cover a wider breadth of the population.
The situation is the same anywhere else — no country has enough cholera vaccines today. This shortage is not going to be solved soon so countries shouldn’t count on vaccination to prevent or curb cholera outbreaks. This stresses the urgency of strengthening water and sanitation systems.
“We just go to the river with our containers and dig a shallow well in the sand. Once we reach the water level, we just wait for a few minutes for the unwanted particles in the water to settle down and then we fetch our water. We then destroy the shallow well by putting sand again on top of the water and we leave. This way we feel the water is safe and our elders have been doing this since time immemorial and none of them has ever complained of any stomach pains.” — Delinah, Buhera
The longer-term solutions include replacing antiquated water and sewage systems, implementing a sustainable waste disposal system, and providing pipes for safe water. The provision of safe water, basic sanitation, and hygiene practices is critical to preventing and controlling the transmission of cholera and other waterborne diseases.
In response to the 2023 cholera outbreak in Zimbabwe, the government and non-governmental organizations launched extensive efforts to combat the disease. These combined efforts appear to be working, but more effort will be needed to get to zero cases. MSF continues to support cholera response around the country.
Caring for patients and enhancing cholera prevention measures are both critical elements to bringing the outbreaks under control. But without meaningful action to ensure people’s access to safe drinking water, cholera is likely to resurface regularly in the country.
MEDICAL doctors are pushing for an independent regulatory body that has no links to the government, similar to the lawyers’ Law Society of Zimbabwe.
This emerged during discussions on the proposed amendments to the Health Professions Act, with doctors insisting that the move will ensure high professionalism in the health sector.
The meetings were convened by the Zimbabwe Association of Doctors for Human Rights in conjunction with the Zimbabwe Lawyers for Human Rights, the Southern Africa Parliamentary Support Trust, the College of Primary Care Physicians of Zimbabwe, the Zimbabwe College of Public Health Physicians and the Zimbabwe Medical Association.
Doctors and nurses attended the meetings, which were held in Harare, Gweru and Bulawayo recently.
The doctors argue that they do not want government interference with the activities of the Health Professions Council institutions.
They also disapprove of the amendment of Section 26, which proposes the closure of health facilities for non-payment of subscriptions, which they said infringed on the right to health.
They have also expressed concern over the late issuance of practising certificates by the authorities after payment of subscriptions, insisting that the regulatory authority should issue certificates within seven days.
The doctors also argued that the amendment of Section 30 forces them to do research.
They argued that research should be optional and be pursued by those who wish to be academic and those who want to work should not be subjected to forced research.
“[There] is an attempt by government to take control of Health Professions Council institutions, particularly the finances of the councils,” they claimed.
“The fees that the different councils are charging are also exorbitant and do not match the service that members get as they sometimes get their practising certificates towards the end of the year [yet] they would have paid subscriptions beginning of each year.
“Rather than the soft language proposed, there should be a closer look into the running of the funds of each council and accountability mechanisms to the members … there is ambiguity because of the terminology that was used … the use of non-financial terms like evaluate and act upon is ambiguous and leaves room for nefarious activities happening.”
The medical professionals also shot down the proposal to rename the Nurses Council of Zimbabwe to Nurses and Midwives Council of Zimbabwe, arguing that there were other categories of nurses other than midwives, so the name should represent all the categories.
The health professionals, who proposed a rotational system for the presidency of the Health Professions Council, also pointed out: “The clause on appeals implies that the decision of the (Health Professions) council will stand until an appeal is heard …under normal circumstances, an appeal should suspend the decisions made until the matter is heard.
“The clause in its current form violates principles of natural justice as well as rights of citizens as enshrined in the Constitution. Since legislation can sometimes be used for social engineering, members noted that the clause may be used politically and deny justice to health professionals.”
The health professional complained of “multiple registrations required by government, which costs money and time”.
There is need to harmonise registrations as part of the ease of doing business,” they said.
Another bone of contention the doctors expressed concern about is government’s ban on job actions lasting more than three days at a time when the health sector is saddled with a myriad of challenges, among them poor remuneration and working conditions.
The doctors described the Amendment Bill as “neither democratic nor consultative”, with the nurses weighing in saying that public health sector workers “are now disadvantaged in several ways because they have no right to strike and they cannot engage in collective bargaining”.
Also under the new law, worker representatives who are charged with inciting nurses and doctors to unlawfully down tools could be jailed for three years which authorities argue is necessary to “instil discipline” in the health sector.








































Recent Comments