
UNICEF Zimbabwe Polio Response Situation Report No. 1 for 02-16 February 2024
on February 19, 2024 in News, Press Statements

Highlights
- Zimbabwe detected seventeen (17) circulating vaccine derived polio virus type 2 (cVDPV2) from environmental samples in Harare since October 2023. The samples were from four polio environmental surveillance sites in Harare.
- Polio outbreak was declared a public health emergency (PHE) by the Minister of Health and Child Care in October 2023.
- An index human cVDPV2 was reported in a 10-year-old female AFP case in January 2024.
- Two newly confirmed AFP cases (samples from contacts) have been reported this week (cumulative 23) with a NPAFP rate at 1.3 per cent children over 15 years.
- A total of 10,517,500 doses of nOPV2 were received on 29 January 2024 for the planned two supplementary immunization activities (SIAs). Expiry date 14/08/2025.
- A joint press release on Round 1 national nOPV2 polio SIA done by the Honorable Deputy Minister of Health and Child Care (MoHCC) with UNICEF, WHO and Partners on 16 Feb 2024.
Situation Overview & Humanitarian Needs
Zimbabwe last reported a case of indigenous wild polio virus (WPV) in 1986 and had been certified polio free in 2005.
Following the detection of WPV1 in Mozambique and Malawi, in 2022, Zimbabwe also undertook the multi-country supplementary immunization activities (SIAs) with bOPV2 and managed to conduct four rounds of SIA.
In 2023, Zimbabwe detected seventeen circulating vaccine derived polio virus type 2 (cVDPV2) from environmental samples in Harare since October 2023.
The samples were from the 4 polio environmental surveillance sites in Harare.
Two newly confirmed AFP cases (samples from contacts) have been reported this week (cumulative 23) with a NPAFP rate at 1.3 per cent children >15 years.
The cVDPV2 outbreak was declared a public health emergency by the Minister of Health and Childcare (MOHCC) in October 2023.
Polio outbreak response activities commenced with plans to conduct two supplementary immunization activities (SIAs) using novel oral polio vaccine type 2 (nOPV2) starting 20 February 2024.
The risk of poliovirus spreading within the country and neighboring countries remains high.
Special considerations need to be made in the polio outbreak response for special populations who include vaccine hesitant religious groups who are densely populated in Manicaland (Buhera, Mutasa and Mutare districts), populations in refugee camps (Tongogara in Manicaland and Waterfalls transit camp in Harare), populations along borders, cross border traders, artisanal miners, and populations in emerging peri urban settlements in Harare.
SOURCE:: ReliefWeb via link https://reliefweb.int/report/zimbabwe/unicef-zimbabwe-polio-response-situation-report-no-1-02-16-february-2024

UNICEF supports Zim’s Integrated Approach in the Battle Against Cholera
on February 9, 2024 in Cholera, News, Press Statements
Empowering Communities: Ensuring access to safe water and promoting public awareness on cholera prevention

Zimbabwe is currently grappling with a cholera outbreak, with more than 22,000 recorded cases and over 500 suspected and confirmed deaths.
The widespread impact of the outbreak has touched every corner of the country.
UNICEF is actively supporting the government-led response to the cholera crisis on multiple fronts, treatment of cholera-infected people, initiatives to provide access to safe water, disseminating preventive messages, and advocating for seeking medical support in case of infection.
To address the urgent needs of affected communities, UNICEF supplies critical items such as water purification tablets, hygiene kits, soap, and water containers.
These essentials play a crucial role in ensuring communities have access to clean water and can uphold proper sanitation practices.
Additionally, UNICEF is actively involved in the cholera vaccination campaign and the implementation of public awareness activities, designed to inform communities about cholera’s causes, preventive measures, and the significance of hygiene practices.
Emphasising community participation, UNICEF collaborates with local leaders, influencers, and health workers to effectively communicate key messages and engage communities in the prevention and response efforts against cholera.

A Learner from Glen View 7 primary school in school in one of the cholera hotspots in Harare is washing their hands using UNICEF supported handwashing station
More than 260,000 people have been reached with critical WASH [water, sanitation and hygiene] supplies, including the distribution of over 1,200 handwashing stations in schools in hotspot areas as part of the back-to-school campaign.
The supply of non-food items (NFIs) ensures that children learn in a safe environment to promote access to quality education.
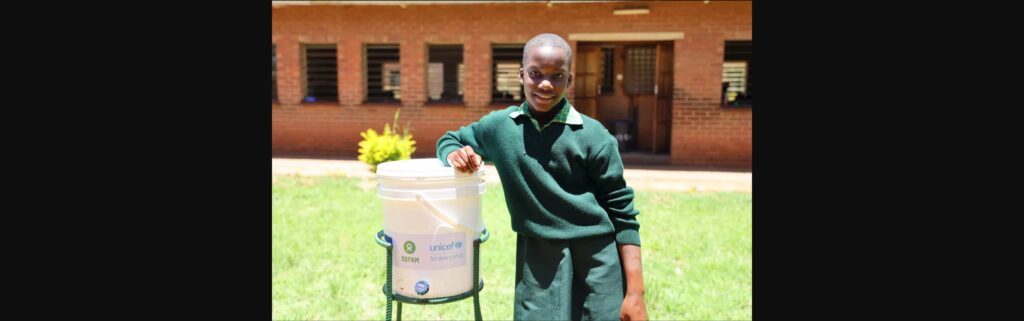
A learner from Glen View 7 Primary School, in school in one of the cholera hotspots in Harare, standing beside UNICEF supported handwashing station
As part of the back-to-school campaign over 10,000 school children were the recipients of key hygiene messages on cholera and its prevention via Rapid-Pro.
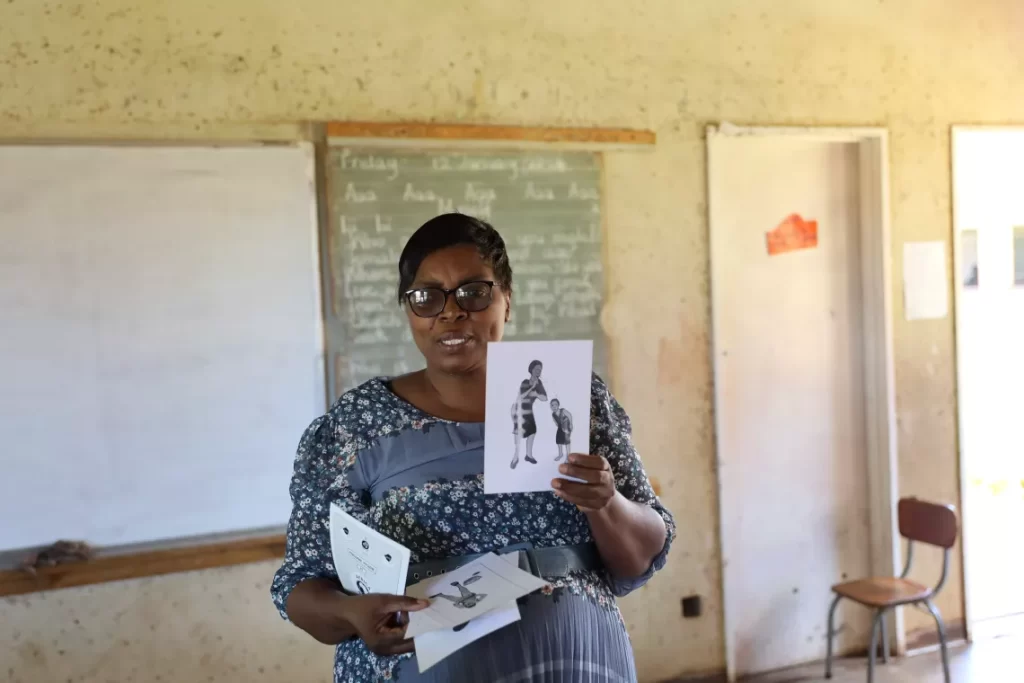
Priscilla Chimbwanda (56), School Health Coordinator uses visual cards to deliver key messages on hygiene messages and Cholera prevention to a classroom full of students
School Health Coordinators have been integral to the back-to-school activities, trained by UNICEF and partners in collaboration with the Ministry of Primary and Secondary Education on essential hygiene messages for cholera prevention.
This ensures a comprehensive approach to addressing cholera within the school environment.

A Community Health Promoter from Glen View, a cholera hotspot area in Harare, delivers door-to-door campaign to deliver key hygiene and cholera prevention messages and the distribution of critical supplies
Community Health Promoters are conducting door-to-door campaigns delivering key hygiene and Cholera prevention messages and the distribution of critical supplies.
UNICEF in collaboration with the Ministry of Health and Child Care, trained over 2,2200 health workers, including Community Health Promoters on household case management, community disease surveillance and treatment of patients.
Health workers play a crucial role as a link between the community and the ongoing efforts.

Pepukai Moyo (21) receives Oral Rehydration Solution (ORS) for her 9-month-old son from Oral Rehydration Point in Kuwadzana, a Cholera Hotspot area in Harare.
The Ministry of Health and Childcare, UNICEF and partners established more than 90 oral rehydration points in hotspot communities nationwide, for rehydration of suspected cholera cases to reduce fatality.
Mothers and their small children, pregnant women, people with disabilities, the elderly, and the chronically ill can now readily interact with facility in community.

Community Health Promoter holding water guard chlorination and litmus paper to conduct testing of household water chlorination levels.
As part of ongoing efforts in the Cholera response, UNICEF and partners capacitated and equipped Community Health Promoters to conduct free residual chlorine testing.
UNICEF is promoting household chlorination to increase access to safe water.

Community Health Promoter, Perpetua Maposa (60) from Kuwadzana, a Cholera hotspot area in Harare, conducts bucket chlorination at a community borehole.
To promote access to safe water, UNICEF has facilitated chlorination of water being collected at community boreholes through Community Health Workers.
More than 200 000 litres of water collected at community boreholes in cholera hotspot suburbs in Harare was made safe through the bucket chlorination approach.

Yvonne Mataranyika (73) receives oral rehydration solution at the Oral Rehydration Point (ORP) in Kuwadzana, a Cholera hotspot area in Harare
UNICEF’s cholera response is funded by multiple donors, including the Centre for Disease Control and Prevention (CDC); the European Civil Protection and Humanitarian Aid Operations (ECHO); the Health Resilience Fund (HRF), a Zimbabwean pooled fund supported by the Governments of Ireland, the United Kingdom, the European Union, and GAVI, the Vaccine Alliance; Japan; the UN Central Emergency Response Fund (CERF) and UNICEF Global Humanitarian Funding, and with in-kind support from private sector partners such as Alliance Media & JCDecaux for digital billboards, and Cash-In-Kind logistics support for commodities from Universal Postal Services (UPS).
SOURCE:: Unicef via https://www.unicef.org/zimbabwe/stories/unicef-supports-zimbabwes-integrated-approach-battle-against-cholera

PRESS RELEASE: Zim launches cholera vaccination to curb the spread
on January 30, 2024 in Cholera, News, Press Statements

Target is to vaccinate 2.3 million people in most affected districts
Harare, 29 January 2024 – Today, the Government of Zimbabwe launched a vaccination campaign against cholera, in collaboration with UNICEF and the World Health Organization (WHO). The first cholera vaccines were administrated by the Health and Child Care Honorable Minister Dr Douglas Mombeshora during an event in Kuwadzana, one of the most affected areas of the current cholera outbreak, in the presence of Dr Tajudeen Oyewale, UNICEF Representative, and Professor Jean-Marie Dangou, WHO Country Representative. These vaccines were made possible thanks to the financial support from GAVI, the Vaccine Alliance, whose commitment to global health equity has been instrumental in providing access to life-saving vaccines for Zimbabwe. The cholera vaccines are an additional strategy the Government is rolling out to contain the spread of cholera in Zimbabwe.
Zimbabwe has recorded more than 20,000 suspected cholera and more than 400 confirmed and suspected deaths, since the first cases were recorded nearly a year ago.
A multisectoral cholera response plan led by the Ministry of Health and Child Care Care in collaboration with other government ministries and supported by UNICEF, WHO and partners and donors, has been rolled out focusing on streamlining response co-ordination at all levels, treatment of infected people and prevention of the spread of the disease through improved access to safe water, sanitation, personal and food hygiene and the dissemination of preventive messages to population most at risk.

The introduction of the cholera vaccine is another tool to prevent the further spread of the disease.
The first three batches of 892,286 cholera vaccines arrived via air freight on January 25 and January 27 at Robert Gabriel Mugabe International Airport, from which they were immediately dispatched to be used in the most affected districts in the country.
More arrivals are planned in the days to come.
The cholera vaccine used in Zimbabwe is the Euvichol-Plus vaccine, produced by EuBiologics. It is an oral vaccine administrated by mouth. One dose of vaccine protects against cholera infections for a period of at least six months.

The cholera vaccination campaign in Zimbabwe is targeting 2.3 million people, aged one year old and above, living in 160 wards within 26 high risk districts in 7 provinces: Harare, Mashonaland West, Mashonaland East, Mashonaland Central, Manicaland, Masvingo and Midlands.
These districts are considered the main drivers for the outbreak.
The main operational strategy used in this campaign is house-to-house to minimize gatherings and further spread of the disease.
This is complemented by fixed vaccination points in all health facilities within the catchment area.
Each vaccination team is composed of three people, expected to vaccinate an average of 150 persons per day.

Ahead of the start of the vaccination, a comprehensive social mobilisation campaign was rolled-out to sensitize the population and generate demand for the vaccine.
While the cholera vaccine provides additional protection against infections, it is important to highlight that it does not replace the other cholera prevention measures, like for instance regular hand washing under running safe water, drinking treated or boiled water, safe disposal of solid, liquid, and human waste, and observing food hygiene standards.
SOURCE:: WHO via ling https://www.afro.who.int/countries/zimbabwe/news/press-release-zimbabwe-launches-cholera-vaccination-curb-spread

Rising HIV treatment failure in Zimbabwe: A stitch in time could save nine
on August 25, 2023 in News, Press Statements

Martha Tholanah
“Veld fires start from glowing ash: The numbers dismissed today as small, can offset the gains made in the national HIV response in the near future.”
By Catherine Murombedzi
(Internews Health Journalism Network, Mercury Phoenix Trust HIV/AIDS 2023 Fellowship)
ZIMBABWE should set aside domestic financial resources to deal with the rising number of people living with HIV (PLHIV) resistant to the treatment of first resort, commonly known as the first line treatment.
Donors do not fund second and third line treatment drugs, making this a key health priority for the country. There is no fourth line treatment: If the third line treatment fails, one develops full-blown Aids and, eventually, dies.
Nationally, those on third line on June 30, 2022 were 499, as of June 2023, a total of 533 an increase of 34. In 2018, only 36 patients were on third line treatment.
In June 2023, the second line treatment had 48 937, a decrease from 49 946. A total of 1009 could have died or did not come for resupply or lost to follow up.
The second and third line regimens are purchased using domestic funding. Will my country be able to cater for us if the numbers in need keep growing? I am tired of hunting (for medication) from one clinic to the other because of frequent stockouts,” says Evelyn Chamisa, an HIV patient on second line treatment speaking for many.
The most common reason for changing from first line to second or third line treatment is if the first line treatment fails. Diagnosing HIV is relatively simple these days, yet determining treatment failure is a bit more complex because of different testing methods, challenges patients face in accessing testing centres, and availability of electricity. With an estimated 1.2 million PLHIV – in a population of 15 million – there are concerns over, hence, calls for prompt delivery of viral load testing results.
Viral load testing for HIV is a method that determines the concentration levels of the HIV virus in a person’s blood. The test is used for diagnosis, care, and monitoring a patient’s response to treatment. It may be used to determine whether to keep a patient on first line treatment or to move the patient to second or third lines.
The World Health Organisation (WHO) guidelines recommend that PLHIV take a viral load test twice a year. For many in Zimbabwe, however, a different method – the CD4 count is what they have accessed prior the introductionof viral load testing. CD4 Count measures the damage caused to a person’s protective cells by a virus, bacteria or germ. And this too has been adversely affected over the past three years by the COVID 19 pandemic.
Although the viral load testing method is now available nationally, the results for some patients are never delivered.
Juliet Sanga complains that she has had blood drawn for testing on three occasions, and no results were ever given.
“I have had three tests, and no results were given. I am no longer interested (in further tests),” she says.
Because of Zimbabwe’s frequent electricity shortages, hospitals’ abilities to function properly, including preserving blood samples drawn for tests, are adversely affected. Blood spoils easily, and spoilt blood can not be processed.
Fortunately, the UNDP, financed by the Global Fund, has embarked on a project to power clinics and district hospitals. The project, dubbed “Solar for Health”, has powered 1,047 health centres out of more than 4,000 centres that require electricity.
Mandimika Blander, 51, was luckier than Sanga. After a number of tests, treatment failure was detected, and she was put on second line treatment, which is now working well.
“My health was restored (after I was placed on second line treatment. I got a new lease of life. My life got back to normal). I am now fit, and I have regained weight,” says Mandimika, whose weight had dropped from 110kg to 67kg before treatment failure was detected and reversed through second line treatment.
Still, the shortage of second line treatment drugs is a constant worry for many. Chamisa has, at times, been asked to go drug-hunting when drugs run out in the health facilities. This worries her as she becomes a treatment beggar for her lifeline treatment.
“I had severe side effects when I was on the first line treatment. At one time, I was admitted at Sally Mugabe Central Hospital and tests detected treatment failure. I was placed on the second line. My health improved, and I gained weight. However, the treatment is always in short supply, and when not in stock, I have to (hunt for and) buy, it is very expensive.”
Further, the COVID 19 pandemic added a layer of complications to the lives of PLHIV, heightening fears of treatment failure occurring. For one, access to treatment – whether first line, second line, or third line – was adversely affected as police demanded to see a travel permission note. PLHIV were stigmatized as evidence of travel permission meant disclosure of their HIV status. Many people opted to stay at home rather than face the stigma of public display of their status and drugs. Non-adherence to drugs is a key cause of drug resistance and treatment failure. Speculatively, therefore, the numbers of patients on second – and third line treatment might have been spurred by the COVID 19 pandemic.
Linda, who prefers to use her first name only, had a forced treatment break during the COVID 19 pandemic. She worked as a house help for a middle-class family in Zimbabwe’s capital, Harare.
“When President Emmerson Mnangagwa announced a national lockdown on March 24, 2020, I had three months’ (worth of drugs) supply. I assumed that the lockdown would be lifted before I ran out of doses. This was not to be. I asked my employer for permission to go for a restock. She told me that I was free to collect my medication but never to return. She was afraid I would come back with the COVID-19 virus.”
Between non-adherence due to disruptions caused by COVID 19, being restocked by an activist good Samaritan (Gumisayi Bonzo), joining a WhatsApp support group, losing her job anyway regardless of not leaving the home of her employer, and the official end of COVID 19 as a public health emergency of international concern (PHEIC), Linda was diagnosed with treatment failure and had to be put on second line treatment.
Gumisayi is a founding member and Director of Transmart, an organisation championing the cause of the marginalized transgender community in Zimbabwe. Gumisayi took humanitarian drug-delivery service to people living with HIV during lockdowns triggered by the pandemic in Zimbabwe.
“By January 2023, I had massive weight loss. After different tests – liver function, kidneys, full blood count, CD4 count, viral load test, cervical cancer screening, and tuberculosis (TB) – I was told I had treatment failure and would be moved to the second line treatment. The medical officials emphasized the need to adhere to treatment religiously,” Linda says.
In her own view, this widow with children in high school and an aged mother to take care of, was back to square one, if not worse.
Dr Enerst Chikwati, Country Programme Manager, Aids Healthcare Foundation (AHF) says the rising treatment failure numbers could be attributed to many reasons: From missed doses (non-adherence), to lack of or poor or non-use of effective diagnostic tools to a shortage of health personnel.
“There has been an increase in the number of patients needing third line treatment,” says Dr Chikwati adding, “however, this could be due to increased availability of viral load testing, which has made us see more patients with a high viral load. Also, the on-going training of health care workers has increased coverage of testing services and discovery of drug resistance and, therefore, increased demand.”
Dr Chikwati acknowledges that the main cause of treatment failure is drug resistance as a consequence of poor adherence over the years. “But other factors such as under-dosing in children, drug-to-drug interactions, and other structural factors come into play,” he adds.
He points out that when children’s doses are out of stock, centres issue adult doses, informing parents and guardians to break the tablets before administration. This is risky as it could result in either overdosing or under-dosing and, eventually, treatment failure.
Dr Chikwati emphasizes the need for treatment literacy among patients.
“Educate patients well so that they understand the importance of adhering to the lifelong treatment. Empower health-care workers so that they are better able to manage patients at all levels and detect early treatment failure and intervene. Also, strengthen enhanced adherence counselling to patients,” emphasises Dr Chikwati.
AHF runs five centres of excellence as partners to Zimbabwe’s Ministry of Health and Child Care (MoHCC), offering comprehensive diagnosis, treatment, care, and support reaching 280 PLHIV.
Dr Cleopas Chimbetete, an HIV and Aids specialist at Newlands Clinic, Harare, a centre of excellence in HIV care with over a decade of service, concurs that poor adherence is the reason for the majority who are moved from the first line treatment for the second and third lines: “The only other way that one can have treatment failure, yet they have never missed a dose, is when they get re-infected, cross-infection can cause treatment failure. We urge PLHIV to always use protection. If they get a drug-resistant strain from a partner during sexual intercourse, it means the treatment in force will not work. So always condomize,” advices Dr Chimbetete.
But he emphasises adherence as well as avoiding substance abuse.
“We need to address the issue of poor adherence. About 90 percent of people on second and third line treatment missed their doses of the first line regimen. Young people, especially, struggle to take drugs as prescribed. Substance and drug misuse is also a contributor to lack of adherence. With mutoriro (chrystal meth) misuse, for instance, we notice a rise in young people failing to adhere to treatment,” he says.
Jordan Jani, a drug addict , agrees. He says, “I did not deliberately miss taking my treatment, I was drunk. I blame my friend who had me addicted to mutoriro after high school. I am trying to adhere to treatment now because I am on third line.” He looks forward to a long-acting HIV treatment injectable (as it reduces daily adherence pressures).
“If it delays,” he adds despairingly, “we, the youth, are surely going to die.”
Substance abuse is a growing public health concern in Zimbabwe with young people using anything from cough syrup, a powder from light bulbs, fermenting foods, and extracting a substance from disposed diapers.
According to Dr Nemache Mawere, the Chief Executive Officer at Ingutsheni Psychiatric Hospital, substance abuse has repercussions beyond causing non-adherence to HIV treatment: “For every 12 mental health admissions at our centre, nine are a result of substance abuse. Majority of the users are young people.”
Besides substance abuse, there are other causes of non-adherence, and therefore, treatment failure. A doctor at Sally Mugabe Referral Hospital, Harare, speaking on condition of anonymity as he is not authorised to speak to the media, says belief in faith healing is also to blame for treatment failure.
“I have worked in a public hospital for 15 years. The greatest reason for missed doses stems from faith beliefs, with Pentecostal churches taking the lead. The majority of treatment failure admissions we see wear arm bands inscribed with their leaders’ mantra: ‘By your faith you are healed’.”
The National AIDS Council (NAC), in partnership with the Ministry of Health and Child Care (MoHCC), and partners, run awareness training for all sectors. The faith sector, especially the Apostolic sub-sector, is warming up and beginning to seek health care. In the past, this was not the case; faith healing reigned.
However, Martha Tholanah, a key populations advocate through Making Waves Network, cautions that the one-size-fits-all approach should be discarded. She advocates for treatment that is tailored to individual needs according to circumstances.
“Some people who fail treatment don’t miss doses. Everyone is started on the same regimen. No tests are done to assess if the treatment is suitable. Periodical testing to determine if the treatment an individual is receiving is still appropriate is not done. For example, some council clinics and government hospitals now focus on annual viral load testing and no longer carry out the CD4 Count tests. Yet, if a CD4 Count and other tests were still regularly carried out, together with the viral load testing, one could be moved to other options in the first line before being switched to second line,” Martha says adding, “Veld fires start from glowing ash: The numbers dismissed today as small can offset the gains made in the national HIV response in future.”
Dr Owen Mugurungi, National Director, Aids and TB programme, MoHCC, downplayed the numbers on second and third line treatment, saying it was normal considering the population size.
“A total 499 out of 1.2 million is not worrisome. We have to increase our domestic funding, though, even for our first line regimen.”
NAC Chief Executive, Dr Bernard Madzima, had promised to respond to questions sent to him by email. However, by the time of publishing this article, he had not.
To date, Zimbabwe has contributed US$3.11 million to the Global Fund (GF), from a pledge of US$4.16 million. The country pledged US$1 million for the Global Fund’s Sixth Replenishment, covering 2020-2022. Zimbabwe is both a donor to the Global Fund and an implementer of the Global Fund-supported programmes.
The Aids Levy, which is the domestic funding of 3 percent of a formally employed worker’s taxable income, at its peak, harvested US$38 million in 2013 when the country had dollarised during the Government of National Unity. Since then, the home kitty bag has been waning as the use of the local currency was reintroduced. With the second and third line treatment being funded by the AIDS Levy, the increasing numbers are a cause of concern.
With the average cost per patient annually ranging from US$68 for first line to US$1,000 for second and third lines, the growing numbers on these regimens could give Zimbabwe a headache in the future.
Zimbabwe has 10 provincial hospitals in 10 provinces, with two main referral hospitals. All district hospitals now have state-of-the-art laboratory facilities. Zimbabwe has 59 districts, and currently, 27 districts have hospitals, with five under construction.
A stitch in time saves nine. If Zimbabwe paid attention to the increasing numbers of PLHIV on second and third line treatment, a crisis could be averted!
Source: Health Times






Masvingo residents and health stakeholders attending a Political Dialogue on Health Policy Proposals at Chevron Regency Hotel in the city tonight. There are representatives from Zanu PF, Citizens Coalition for Change and the National Constitution Assembly.
on August 2, 2023 in News, Press Statements






ZADHR MAKES COVID-19 PPE DONATION TO GWERU INFECTIOUS DISEASES HOSPITAL
on April 27, 2021 in COVID-19, News, Press Statements
On Friday April 24, 2020, the Zimbabwe Association of Doctors for Human Rights (ZADHR) supported Gweru Covid-19 isolation facilities with personal protective equipment and hygiene material towards the fight against Covid-19 in the Midlands capital. Executive director Mr Calvin Fambirai led the ZADHR delegation, while Gweru city health director Dr Samson Sekenhamo received the donation on behalf of the city. The donation included infrared thermometers, B/50 surgical face masks, reusable face masks, face shields, B/100 latex gloves, medical gowns, gumboots, N95 masks, caps, goggles, sanitisers, handwashing soap, brooms, water buckets, mops and methylated spirit.











Zadhr 21st Covid-19 Monitoring and Advocacy Report – 5 January 2021
on January 6, 2021 in COVID-19, COVID-19 Monitoring Reports, News, Press Statements
21stCOVID-19 Monitoring and Advocacy Report:
05 January 2020
To date, the World Health Organization (WHO) has recorded over 86,777,613 confirmed cases of COVID-19 and 1,873,855 related deaths. The Ministry of Health and Child Care (MOHCC) in Zimbabwe has reported a total of 17,194 confirmed cases, 418 deaths and 11,813 recoveries of COVID-19 (MOHCC COVID-19 SitRep: 5 January (2021). Harare and Bulawayo seem to be the COVID-19 hotspots in the country, with the two provinces having approximately 54% of the COVID-19 cases. The case fatality rate (CFR) in Zimbabwe is 2.42, which is slightly higher than the CFR for the world cases, which stands at approximately 2.1. This week, the country recorded its highest daily increase in COVID-19 cases (1365), and with the numbers expected to continue to rise, there is need to be more vigilant and urgently align our response strategies in view of these new challenges. On 05 January, the MOHCC SitRep also recorded an unprecedented 34 deaths in a period of 24 hours.
ZADHR continues to monitor the COVID-19 situation in Zimbabwe, providing constructive critiques of the national response and making key recommendations as part of its efforts to help mitigate the unprecedented challenges posed by COVID-19. In this brief, ZADHR pays special focus to the following specific issues:
- Lockdown
ZADHR takes cognisance of the enactment of Statutory Instrument (SI)10 of 2021, Public Health (Covid-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment) Order, 2021 (No. 9). The SI, whose broader mandate is to restore the lockdown in response to the surge in COVID-19 cases, came into effect on the 5th of January 2021.
ZADHR is of the position that the current lockdown measures announced by government, though welcome, may not provide the much-needed impact in breaking the COVID-19 chain of transmission and help in flattening the COVID 19 curve. In a snap survey conducted by ZADHR on the 1st day of the lockdown, many non-essential retailers were in operation across the country. Additionally, human traffic was witnessed at the country borders and in inter-provincial travels. ZADHR posits that there are too many loopholes on the proposed letters of travel authorization process with reports that some retailers were being granted exemption letters to operate in unclear circumstances. We reiterate that the scientific basis of a lockdown is predicated upon limiting most if not all human movement for a period of 14 to 21 days. Furthermore, the government must identify provincial hotspots and have tailored measures or different levels of the lockdown depending on the incidence of COVID-19. Interprovincial travel must be URGENTLY limited and COVID 19 certificates may be considered for all local travel from all COVID-19 hotspots. ZADHR also laments the continued influx of travellers through air when the country is faced with an existential threat of new strains of COVID-19 from South Africa and the UK. The response by the government since the onset of the pandemic has been mostly reactionary and is devoid of proper planning processes that respond to the existing risk levels. ZADHR’s considered view is that the government could have acted proactively and timeously before the festive season to curb movement from both within and outside Zimbabwe. With countries like the United Kingdom and South Africa dealing with the vicious new COVID-19 variant and the high numbers of travellers during the festive season from these two countries, stricter measures were supposed to have been put in place prior to the holidays.
- Re-opening of Schools for Examination Classes
ZADHR acknowledges the move to allow only examination classes to write examinations. However, with the current trends and mutation of the COVID-19 virus, ZADHR suggests that schools should remain closed until the widespread community transmission is under control. ZADHR, encourages the Ministry of Primary and Secondary Education (MoPSE) and all relevant stakeholders to utilise the lockdown and the closure of schools to equip schools with necessary materials and equipment to curb COVID-19 transmission in schools. Treasury must urgently avail the necessary resources to MoPSE and ensure the Standard Operating Procedures (SOPs) for the Safe Re-opening of Schools are implemented expeditiously.
- Public Compliance and Enforcement of Regulations
ZADHR notes that the previous lockdown was marred by several cases of human rights violations allegedly perpetrated by State security agents deployed to enforce lockdown and other COVID-19 regulations. ZADHR continues to reiterate the importance for a rights-based approach to enforcement of regulations which provides for the respect and promotion of civil and political liberties as enshrined in the constitution and international human rights instruments. ZADHR warns the government against excessive use of force, arbitrary arrests or detention, torture or any other cruel or inhumane treatment for those breaching lockdown regulations. ZADHR also implores the public to follow the stipulated regulations to help compliment the efforts of the Government towards the fight against COVID-19.
- Equity
ZADHR notes with concern the absence of strong and robust social safety nets to support the vulnerable, indigent, and marginalised communities such as the elderly, disabled and other vulnerable populations. Policies designed to curtail movement have impact on the livelihoods of poor individuals and communities, who generally depend on day-to-day enterprising, thus demanding COVID-19 response strategies that have a binary approach which involves cutting transmission models and complementing the poor with necessary social and economic support to enhance their livelihoods and well-being.
- Provision of PPE
ZADHR is gravely concerned with the continued increase in the number of health professionals who are being infected with COVID-19 during the discharge of their duties. Our conservative estimates, points towards over 1 000 health workers being infected with COVID-19. Medical associations have continued to highlight the worrying trends of health workers working without adequate PPE. We reiterate that the unavailability of PPEs is a violation of the 2020 High Court ruling (ZADHR vs Ministry of Health and Child Care and Others) which directed government to provide adequate PPE to all frontline health workers and also is against the tenets of the International Labour Organisation (ILO) Decent Work Agenda. ZADHR will soon be seeking enforcement of the court resolutions in its efforts to ensure adequate protection of health workers.
- Testing and Screening
The current testing statistics are not in tandem with the rising burden of COVID-19. The positivity rate in the few tests done over the past few days has been averaging 20%, highlighting the possibility that the pandemic could be much worse than what is reflecting in the MOHCC SitReps. Furthermore, the proximity and increased travel between Zimbabwe and South Africa calls for Zimbabwe to also investigate the genomic structure of the COVID-19 cases we are witnessing URGENTLY. The public health approach must then be tailored depending on whether we are dealing with a more transmissible strain of COVID 19 or not.
- Hospitalisation -ICU and IDU Increased Capacity
ZADHR notes with concern the limited capacity of local health facilities to accommodate cases that need hospitalisation. The continued surge in new infections has caused the hospitals to be overwhelmed and fail to cater for the increased number of COVID-19 related hospital admissions. ZADHR condemns in the strongest terms possible the sad situation of continued limited ICU capacity almost ten months after the detection of the 1st COVID-19 case. We reiterate that government has an obligation to ensure availability of emergency medical care to all Zimbabweans as stipulated in Section 76 of the constitution.
- Training and Capacity Building of Health Workers
There is need for ongoing training of health workers on case definition, case management and how they adequately respond to the possibility of a new COVID-19 variant/ strain. The government should continue to invest in building the capacity of health workers, nurses, doctors and primary health workers. Zimbabwe is likely to have a more nationwide spread of COVID-19 and there is need for other cadres like primary health care workers in rural health centre who were not previously involved in the management of COVID-19 cases to be capacitated.
- COVID-19 Vaccine
ZADHR implores the government to urgently outline its vaccine roll out and distribution plan. We further call upon the MOHCC to guarantee that it will make efforts to ensure the availability of a safe, effective and free vaccine to most Zimbabweans and the tenets of equity will be applied to prioritize high risk and vulnerable groups. ZADHR urges the government to come dissuade against some sectors of the society who are promoting COVID 19 vaccine hesitancy. To prepare for the vaccine, there is need to revamp health system infrastructure such cold chain facilities in hospitals and clinics, training of health workers and putting in place necessary logistical support needed for an enormous vaccination campaign targeting millions of Zimbabweans.
- Information Dissemination
Finally, ZADHR calls for the government to be more accountable and communicate effectively on the COVID 19 situation in the country. The key figures in the COVID-19 response must continuously address the public on key and emerging issues on the response to ensure that there is no information gap between the government and the public.
21stCOVID-19 Monitoring and Advocacy Report:
05 January 2020
To date, the World Health Organization (WHO) has recorded over 86,777,613 confirmed cases of COVID-19 and 1,873,855 related deaths. The Ministry of Health and Child Care (MOHCC) in Zimbabwe has reported a total of 17,194 confirmed cases, 418 deaths and 11,813 recoveries of COVID-19 (MOHCC COVID-19 SitRep: 5 January (2021). Harare and Bulawayo seem to be the COVID-19 hotspots in the country, with the two provinces having approximately 54% of the COVID-19 cases. The case fatality rate (CFR) in Zimbabwe is 2.42, which is slightly higher than the CFR for the world cases, which stands at approximately 2.1. This week, the country recorded its highest daily increase in COVID-19 cases (1365), and with the numbers expected to continue to rise, there is need to be more vigilant and urgently align our response strategies in view of these new challenges. On 05 January, the MOHCC SitRep also recorded an unprecedented 34 deaths in a period of 24 hours.
ZADHR continues to monitor the COVID-19 situation in Zimbabwe, providing constructive critiques of the national response and making key recommendations as part of its efforts to help mitigate the unprecedented challenges posed by COVID-19. In this brief, ZADHR pays special focus to the following specific issues:
- Lockdown
ZADHR takes cognisance of the enactment of Statutory Instrument (SI)10 of 2021, Public Health (Covid-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment) Order, 2021 (No. 9). The SI, whose broader mandate is to restore the lockdown in response to the surge in COVID-19 cases, came into effect on the 5th of January 2021.
ZADHR is of the position that the current lockdown measures announced by government, though welcome, may not provide the much-needed impact in breaking the COVID-19 chain of transmission and help in flattening the COVID 19 curve. In a snap survey conducted by ZADHR on the 1st day of the lockdown, many non-essential retailers were in operation across the country. Additionally, human traffic was witnessed at the country borders and in inter-provincial travels. ZADHR posits that there are too many loopholes on the proposed letters of travel authorization process with reports that some retailers were being granted exemption letters to operate in unclear circumstances. We reiterate that the scientific basis of a lockdown is predicated upon limiting most if not all human movement for a period of 14 to 21 days. Furthermore, the government must identify provincial hotspots and have tailored measures or different levels of the lockdown depending on the incidence of COVID-19. Interprovincial travel must be URGENTLY limited and COVID 19 certificates may be considered for all local travel from all COVID-19 hotspots. ZADHR also laments the continued influx of travellers through air when the country is faced with an existential threat of new strains of COVID-19 from South Africa and the UK. The response by the government since the onset of the pandemic has been mostly reactionary and is devoid of proper planning processes that respond to the existing risk levels. ZADHR’s considered view is that the government could have acted proactively and timeously before the festive season to curb movement from both within and outside Zimbabwe. With countries like the United Kingdom and South Africa dealing with the vicious new COVID-19 variant and the high numbers of travellers during the festive season from these two countries, stricter measures were supposed to have been put in place prior to the holidays.
- Re-opening of Schools for Examination Classes
ZADHR acknowledges the move to allow only examination classes to write examinations. However, with the current trends and mutation of the COVID-19 virus, ZADHR suggests that schools should remain closed until the widespread community transmission is under control. ZADHR, encourages the Ministry of Primary and Secondary Education (MoPSE) and all relevant stakeholders to utilise the lockdown and the closure of schools to equip schools with necessary materials and equipment to curb COVID-19 transmission in schools. Treasury must urgently avail the necessary resources to MoPSE and ensure the Standard Operating Procedures (SOPs) for the Safe Re-opening of Schools are implemented expeditiously.
- Public Compliance and Enforcement of Regulations
ZADHR notes that the previous lockdown was marred by several cases of human rights violations allegedly perpetrated by State security agents deployed to enforce lockdown and other COVID-19 regulations. ZADHR continues to reiterate the importance for a rights-based approach to enforcement of regulations which provides for the respect and promotion of civil and political liberties as enshrined in the constitution and international human rights instruments. ZADHR warns the government against excessive use of force, arbitrary arrests or detention, torture or any other cruel or inhumane treatment for those breaching lockdown regulations. ZADHR also implores the public to follow the stipulated regulations to help compliment the efforts of the Government towards the fight against COVID-19.
- Equity
ZADHR notes with concern the absence of strong and robust social safety nets to support the vulnerable, indigent, and marginalised communities such as the elderly, disabled and other vulnerable populations. Policies designed to curtail movement have impact on the livelihoods of poor individuals and communities, who generally depend on day-to-day enterprising, thus demanding COVID-19 response strategies that have a binary approach which involves cutting transmission models and complementing the poor with necessary social and economic support to enhance their livelihoods and well-being.
- Provision of PPE
ZADHR is gravely concerned with the continued increase in the number of health professionals who are being infected with COVID-19 during the discharge of their duties. Our conservative estimates, points towards over 1 000 health workers being infected with COVID-19. Medical associations have continued to highlight the worrying trends of health workers working without adequate PPE. We reiterate that the unavailability of PPEs is a violation of the 2020 High Court ruling (ZADHR vs Ministry of Health and Child Care and Others) which directed government to provide adequate PPE to all frontline health workers and also is against the tenets of the International Labour Organisation (ILO) Decent Work Agenda. ZADHR will soon be seeking enforcement of the court resolutions in its efforts to ensure adequate protection of health workers.
- Testing and Screening
The current testing statistics are not in tandem with the rising burden of COVID-19. The positivity rate in the few tests done over the past few days has been averaging 20%, highlighting the possibility that the pandemic could be much worse than what is reflecting in the MOHCC SitReps. Furthermore, the proximity and increased travel between Zimbabwe and South Africa calls for Zimbabwe to also investigate the genomic structure of the COVID-19 cases we are witnessing URGENTLY. The public health approach must then be tailored depending on whether we are dealing with a more transmissible strain of COVID 19 or not.
- Hospitalisation -ICU and IDU Increased Capacity
ZADHR notes with concern the limited capacity of local health facilities to accommodate cases that need hospitalisation. The continued surge in new infections has caused the hospitals to be overwhelmed and fail to cater for the increased number of COVID-19 related hospital admissions. ZADHR condemns in the strongest terms possible the sad situation of continued limited ICU capacity almost ten months after the detection of the 1st COVID-19 case. We reiterate that government has an obligation to ensure availability of emergency medical care to all Zimbabweans as stipulated in Section 76 of the constitution.
- Training and Capacity Building of Health Workers
There is need for ongoing training of health workers on case definition, case management and how they adequately respond to the possibility of a new COVID-19 variant/ strain. The government should continue to invest in building the capacity of health workers, nurses, doctors and primary health workers. Zimbabwe is likely to have a more nationwide spread of COVID-19 and there is need for other cadres like primary health care workers in rural health centre who were not previously involved in the management of COVID-19 cases to be capacitated.
- COVID-19 Vaccine
ZADHR implores the government to urgently outline its vaccine roll out and distribution plan. We further call upon the MOHCC to guarantee that it will make efforts to ensure the availability of a safe, effective and free vaccine to most Zimbabweans and the tenets of equity will be applied to prioritize high risk and vulnerable groups. ZADHR urges the government to come dissuade against some sectors of the society who are promoting COVID 19 vaccine hesitancy. To prepare for the vaccine, there is need to revamp health system infrastructure such cold chain facilities in hospitals and clinics, training of health workers and putting in place necessary logistical support needed for an enormous vaccination campaign targeting millions of Zimbabweans.
- Information Dissemination
Finally, ZADHR calls for the government to be more accountable and communicate effectively on the COVID 19 situation in the country. The key figures in the COVID-19 response must continuously address the public on key and emerging issues on the response to ensure that there is no information gap between the government and the public.
///END///
Recent Posts
-
 Brain drain continues to haunt Zim as close to 36,000 are granted work visas to the UK alone in just a year
Brain drain continues to haunt Zim as close to 36,000 are granted work visas to the UK alone in just a year
-
 US$30,8m collected from sugar tax: Govt
US$30,8m collected from sugar tax: Govt
-
 ‘There are no drugs’: Zimbabwe’s sick turn to herbalists over ailing health system
‘There are no drugs’: Zimbabwe’s sick turn to herbalists over ailing health system
-
 Where Is the Sugar Tax Money Going? Doctors Demand Answers from Mthuli Ncube
Where Is the Sugar Tax Money Going? Doctors Demand Answers from Mthuli Ncube
-
 Doctors query sweetness of Ncube’s sugar tax
Doctors query sweetness of Ncube’s sugar tax
Recent Comments