
Village Health Workers engage community influencers to drive demand for health services
on July 17, 2024 in Health and Wellbeing, News, Uncategorized
‘It’s a turnaround.’ A rural hospital credits village health workers and community influencers for transformation in uptake of services

Umguza, Zimbabwe – In a tiny office at Mbembesi rural health facility in Matabeleland North’s Umguza district, Thembinkosi Sibanda, a midwife, took stock of the numbers in the facility’s birth register. A contented smile followed.
Seven deliveries from the hospital’s maternity wing for the month. Only a single home delivery.
These are numbers she would hardly have imagined two years ago.
“We would usually record one or two deliveries here but most pregnant women would deliver in unsafe conditions at home,” said Sibanda, whose facility, surrounded by hard-to-reach rural and resettlement areas, now records between eight and ten births a month.
“It’s a turnaround,” she marveled, and, as if speaking to herself, added, “Job well done.”
Yet, Sibanda refused to take responsibility for the change.
“They are the real heroes, the credit goes to them,” she said, pointing to a group of village health workers (VHWs), local traditional and religious leaders and young people sitting in a shed for an advocacy meeting.
VHWs have forged a transformative partnership with community influencers to increase demand for, and access to primary healthcare services as well as engender improved water, sanitation and hygiene practices.
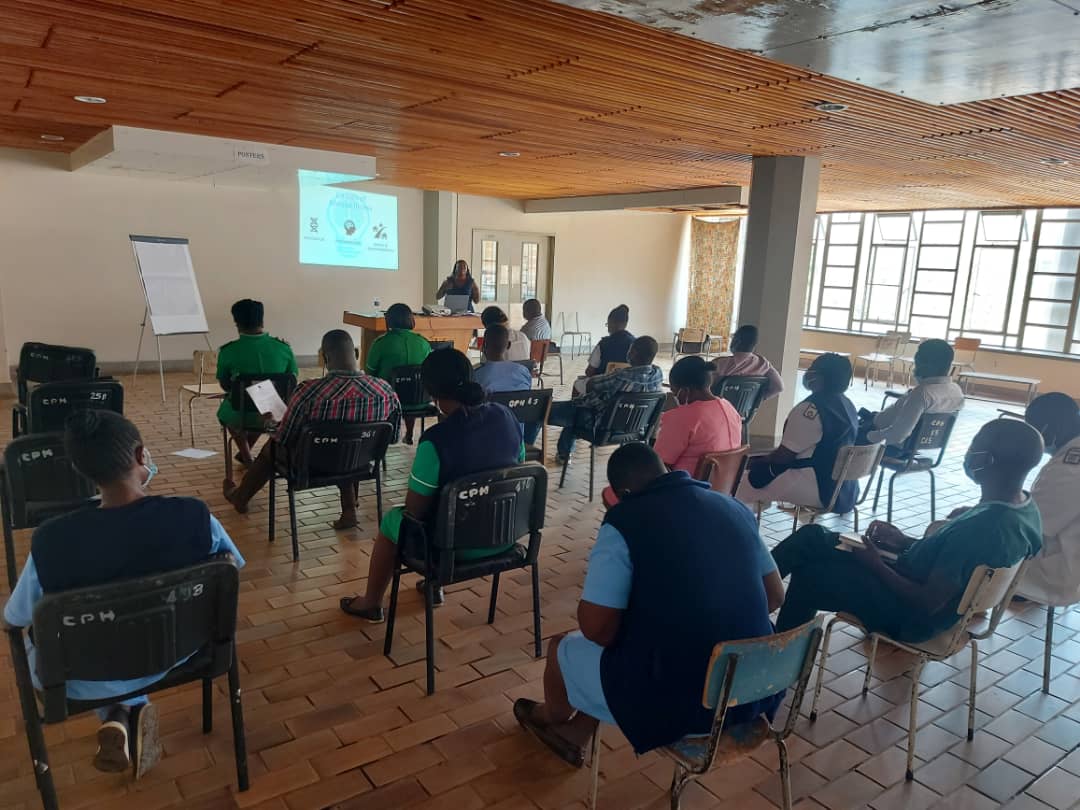
As part of interventions to strengthen primary health care services such as immunization, HIV services, non-communicable disease screening and treatment and health education, over 400 VHWs in 11 districts across several provinces recently underwent refresher training on how to intensify demand for services management and treatment of minor ailments at household level.
One of the results of those sessions, conducted by the Health and Child Care ministry in partnership with UNICEF and with funding from Gavi, the Vaccine Alliance, with funds from the Government of France, is the increased active participation of influential, authoritative, and trusted members of the community in amplifying the work of VHWs.
Authorities held community advocacy meetings with 1,500 key influencers who are trusted members of the community and included VHWs, interfaith and traditional leaders as well as young people such as peer educators to boost demand for COVID-19 vaccination, HPV vaccination, Vitamin A Supplementation and other vaccines amid successive outbreaks of measles, polio and cholera.
The meetings, done at ward and village level in all the 11 districts involved in the project, also discussed issues like demand for neonatal and postnatal care, HIV testing and treatment, COVID-19 self-testing, adolescent health services and how to intensify awareness campaigns.

Village health workers regularly attend refresher training sessions and cascade the information to community influencers who have become key partners in mobilisation and amplifying awareness campaigns
This kind of strengthening of primary health care support has contributed to increased referrals for vaccine hesitant groups and other children facing multiple deprivations.
The VHWs embarked on a journey to update their integrated village registers to record and account for every child in their respective communities and geo coding using ODK on their smartphones.
Out of the 3,879 zero children identified in 2023 in Umguza District, 3,685 – representing 95% – were successfully followed up and vaccinated.
Out of the 9,165 zero dose children identified in 2022 in the urban areas of Harare, Bulawayo, and Chitungwiza, 8,706, representing 95%, were successfully tracked and vaccinated.
The VHWs also recorded 24,424 under immunised children, with the majority referred or accompanied for vaccination.
Health authorities say they are roping in community influencers into some of their regular programmes to sustain the successes.
“Nowadays we also invite the influencers to the monthly meetings that we ordinarily have with Village Health Workers. They have become dependable partners for village health workers in mobilisation and awareness campaigns,” said Sibanda, the midwife at Mbembesi health facility.
Faith leaders have become key pillars in intensifying awareness and uptake of vaccines and other modern medicines among denominations whose doctrines undermine health seeking behaviours.
Traditional leaders such as village heads in the highly patriarchal community are now treating Village Health Workers, who are mostly female, as part of their inner circle.
Sheila Ncube is one of the 19 VHWs providing a link between Mbembesi hospital and people in hard-to-reach communities that are part of the facility’s catchment population of over 8,000 people scattered across the vast district.
With settlements opening up in the area, she needs her village head to point her to new inhabitants, who often lack basic water, sanitation and hygiene infrastructure and are also unfamiliar with health services offered in the area.
“The village head is the one who carries the word when I want people to gather for awareness sessions at a central point or when I am mobilising for campaigns such as vaccination. He is the one who helps me identify pregnant women in the village, he is my eyes and ears,” said the 70 year-old.
One of the village heads at the advocacy meeting, Lucky Sibanda, thinks the compliments belong to the VHWs, whom he describes as his mentors. Sibanda said he was previously indifferent to the services of Village Health Workers – until COVID-19 struck.
“They saved my community,” he said, referring to the VHWs.
“They educated people on prevention and treatment and many people ended up overcoming their fear of vaccines.”
When his local Village Health Worker approached him for help to mobilise for measles, polio, cholera vaccines following the outbreaks, Sibanda gladly obliged.
“The Village Health Worker is now my chief whip. She is always by my side when I hold functions. I have made it a rule that no gathering proceeds before she speaks about health,” said Sibanda. He reckons he is also turning into a campaigner, thanks to his increased interactions with VHWs and health workers.
Ongoing mentorship and coaching that has reached 2,200 health workers and Village Health Workers on issues such as integrated service delivery, data collection, consolidation, analysis and reporting also cascades to community members such as traditional leaders, turning them into cadres.
“She teaches me whatever she would have learned from the workshops she attends. She has equipped me with information so much that nothing escapes me anymore, HIV treatment defaulters, sanitation and hygiene red flags, underweight children and pregnant mothers. I alert her as soon as I notice something amiss,” he said.
Heavy with pregnancy, 28-year-old Polite Ndlovu is one of those grateful for the intervention after being nudged by her village head and Village Health Worker to register her pregnancy at the hospital.

Pregnant women such as Polite Ndlovu are increasingly accessing quality neonatal and postnatal care at health facilities due to awareness spread by Village Health Workers and community influencers
“I planned to go but I was procrastinating but they warned me and other pregnant women in the village about the dangers,” she said.
“I went to the hospital the following day,” added Ndlovu on the grounds of Mbembesi hospital, where she had gone for a routine check-up.
SOURCE:: unicef via link https://www.unicef.org/zimbabwe/stories/village-health-workers-engage-community-influencers-drive-demand-health-services



















































Recent Comments