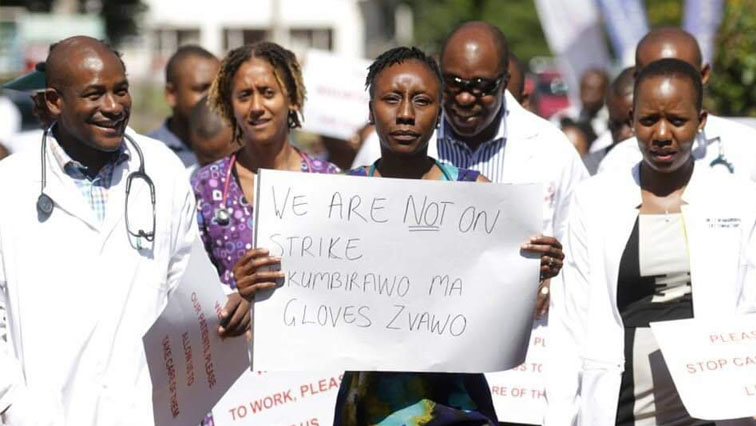
Zimbabwean medical professionals across the country have lamented the dire working conditions within the healthcare sector.
In their statement to mark Workers’ Day on Wednesday, 01 May, the Zimbabwe Association of Doctors for Human Rights (ZADHR) said that doctors are exposed to harm in their line of duty. Reads the statement:
The Zimbabwe Association of Doctors for Human Rights (ZADHR) joins the rest of the world in marking International Workers Day, 2024. This year’s commemorations are focused “on ensuring safety and health at work in a changing climate”. In commemorating this day, ZADHR laments the state of our public health delivery system and the exposure of health professionals to harm in their line of duty. For years, health workers in Zimbabwe have clamoured for a health service and health workplace that promotes and protects their rights through strengthening infection control protocols and associated provisions for infection control such as personal protective equipment. Effective infection control protocols will not only make the workplace a safe place but will contribute to boosting the moral and mental health of health professionals, which have been dented by poor remuneration, dilapidated infrastructure, equipment and shortage of drugs and sundries. In marking this day, ZADHR continues to urge the government to address the health and safety concerns of health professionals to prioritise the health and well-being of health professionals. It is our firm belief that a safe working place is good for the physical and mental well-being of health professionals.
Thousands of Zimbabwean healthcare workers have left the country for countries such as the United Kingdom and Australia due to poor remuneration and working conditions resulting in shortages, particularly in public institutions.
Official statistics indicate that over 4,000 nurses and doctors have left Zimbabwe since February 2021.
AS Zimbabwe celebrated Workers’ Day on Wednesday, medical professionals across the country decried the dire working conditions within the healthcare sector.
The Zimbabwe Association of Doctors for Human Rights (ZADHR) highlighted that medical practitioners are disproportionately affected by the poor state of hospitals nationwide.
“The Zimbabwe Association of Doctors for Human Rights (ZADHR) joins the rest of the world in marking International Workers Day, 2024. This year’s commemorations are focused “on ensuring safety and health at work in a changing climate”.
“In commemorating this day, ZADHR laments the state of our public health delivery system and the exposure of health professionals to harm in their line of duty,” read the statement.
Doctors have repeatedly demanded improvements to their working environments, citing the dangers they face due to inadequate equipment and bad working conditions.
Public hospitals in the country which the majority of citizens rely on are short of medical sundries hindering the effective delivery of services.
ZADHR urged the government to implement concrete measures that will transform Zimbabwe’s healthcare system for the better.
“For years, health workers in Zimbabwe have clamoured for a health service and health workplace that promotes and protects their rights through strengthening infection control protocols and associated provisions for infection control such as personal protective equipment.
“Effective infection control protocols will not only make the workplace a safe place but will contribute to boosting the moral and mental health of health professionals, which have been dented by poor remuneration, dilapidated infrastructure, equipment and shortage of drugs and sundries.
“In marking this day, ZADHR continues to urge the government to address the health and safety concerns of health professionals to prioritise the health and wellbeing of health professionals,” read the statement further.
Although medical professionals warn about risks, DIY midwifery remains alive and well in a country where affordable and accessible institutional options continue to dwindle
(Linda Mujuru/Global Press Journal)
Tatenda Mangwanya and her baby, Nqobile, at their home in Hopley, Harare, Zimbabwe. She gave birth with the assistance of Apolonia Takaedza, a self-trained midwife who runs an informal birth center at her home.
HARARE, ZIMBABWE — In the high-density suburb of Hopley, Tatenda Mangwanya, 16, admires her 2-week-old baby girl to whom she gave birth with the assistance of a self-trained midwife.
She stands by her decision to give birth at home, which she says was the safest for her baby, whom she named Nqobile, a Ndebele name meaning “victor.”
“I was registered at a local clinic in the neighboring suburb of Highfield about 10 kilometres from here, but I was transferred to [the hospital] located farther away from my home because I was underage,” Mangwanya explains.
In Zimbabwe, local health clinics employ midwives who assist women with natural births. But women with riskier pregnancies — such as those who are underage and pregnant for the first time — are advised to give birth at a hospital.
“I would go to the hospital for the usual monthly checkups and hear so many stories about women getting operated on unnecessarily and ill-treated by nurses that I was scared,” Mangwanya says.
(Linda Mujuru/Global Press Journal)
A shrine where pregnant mothers wait to give birth in Hopley, Harare, Zimbabwe.
When it was time to give birth, Mangwanya decided to seek assistance from a local spiritual healer.
Many reasons lead Zimbabwean women like her to give birth in their homes or at church shrines, including the cost of public clinics, long distances to health care facilities and a general belief that they are afforded better service at these sites than at hospitals.
However, medical experts interviewed for this article say such births are often conducted under unsafe conditions by untrained people, putting both the mother and baby at risk.
At 363 deaths per 100,000 live births, Zimbabwe’s maternal death rate is considered moderate to high, according to a classification system developed by the World Health Organization.
Another 32 of Africa’s 54 countries also have moderate-to-high maternal death rates, according to a 2023 report by Zimbabwe Coalition on Debt and Development, a nongovernmental organization that advocates for citizen involvement in public policy.
Zimbabwe is far from achieving the United Nations’ sustainable development goal of lowering the maternal death rate to 70 or fewer per 100,000 live births by 2030 — especially in light of the health sector’s brain drain.
Zimbabwe is currently grappling with a deficit of nearly 30,000 health professionals. Almost 4,500 medical professionals have left the country since 2020, mostly seeking better-paid employment abroad.
Apolonia Takaedza, who helped Mangwanya deliver her baby, practices midwifery out of her house in Hopley.
In Zimbabwe’s public hospitals, it’s common for pregnant women to be asked to provide such supplies as gloves and cotton wool at the time of delivery — and that tends to push people away, she says.
“Some don’t have money or even proper clothing for the baby. … When one is giving birth at the hospital, they are required to buy [these items that] they cannot afford,” she says.
Free maternity care used to be available in Zimbabwe through a program tied to the World Bank, but lack of supplies has led hospitals to increasingly charge patients.
Takaedza adds that some women have beliefs that are not recognized at hospitals, including that vaginal growths lead to infertility or miscarriage, and they prefer to be treated by someone who takes these concerns seriously. She also mentions fear of cesarean sections.
“Some choose to give birth at home to avoid being operated. At home, they are guaranteed a normal delivery.”
Takaedza charges US$25 for her midwife service, the same fee charged for a natural delivery at the nearest local clinic. “It’s always negotiable and payable in installments, and that’s why some prefer my service,” she says.
But she has faced difficult situations which may have been better handled at a hospital.
“A friend who also assists women to give birth came with a woman to me after failing to help her deliver. The baby had already died in the womb,” Takaedza says.
(Linda Mujuru/Global Press Journal)
Apolonia Takaedza, who runs an informal birth center at her house, poses for a portrait in Hopley, Harare, Zimbabwe.
To guard against such occurrences, Takaedza says, she always does an assessment before agreeing to help someone deliver.
“Some have children in breach positions and some situations need the hospital.”
Dr. Mugove Madziyire, an obstetrician, says there are many risks associated with home deliveries.
“Any person supervising labor and conducting deliveries must be trained and certified by a responsible authority.”
He adds that labor and delivery can present complications during and after birth.
“There are also medications to be administered to both mother and baby at the time of delivery which prevent complications, such as excessive bleeding from the mother, bleeding disorders in the baby, and eye infections,” he says.
Donald Mujiri, spokesperson for the Ministry of Health and Child Care, says registered nurses with a minimum of three years of experience are eligible for a free, one-year training in midwifery offered through the ministry.
These trained midwives are eligible for employment in local clinics that perform natural births.
A few kilometers from Takaedza’s residence, Hilda, a member of an apostolic sect, also assists women giving childbirth from her home. Unlike Takaedza, Hilda — who asked to be identified only by her first name as her sect doesn’t allow members to speak to the press — has a waiting shelter for such women; they usually stay at her house from about seven months of pregnancy.
Inside Hilda’s makeshift delivery room, walled with plastic and lined with grass, a young mother smiles as she holds her newborn baby boy, delivered the previous night.
Other pregnant women, also members of the same church, gather around her, congratulating her as they each wait for the day they will deliver.
(Linda Mujuru/Global Press Journal)
Beatrice Zindora, who also runs a birth center at her house, prays at her home in Hopley, Harare, Zimbabwe
Outside, smaller makeshift rooms house 24 other pregnant women, waiting to deliver their babies.
Hilda does not have any medical qualifications — only her practical experience.
The 51-year-old says she started to help women from her church give birth when she was 36, after experiencing a “calling” to do this kind of work.
“I have given assistance to over 400 women. As a rule in our church, we do not go to the hospital for deliveries,” she says.
Hilda says that in 15 years of practice, she has never once had to rush a woman to a hospital. “We do face challenges, but I always get a voice that speaks to me and instructs me on how to deal with each and every situation,” she says.
She adds she also doesn’t use gloves when performing the procedures, “as per church doctrine.” Members of this church are known for distrusting medical practice and vaccines.
Dr. Lucia Gondongwe, deputy director of reproductive health at the Ministry of Health and Child Care, says the ministry upholds institutional deliveries as the standard of care.
“This enables women to get a comprehensive package of care required for childbirth and the newborn,” she says, adding that it ensures both the mother and baby get emergency assistance if it’s needed.
But Edinah Masiyiwa, executive director of Women’s Action Group, an NGO that advocates for women’s rights, says that institutional health care has only worsened during the broader economic decline.
“We are in a situation where the public system is requesting women to bring everything needed for their care — things like pads, methylated spirit, cord clamps,” she says.
“If there is need for a transfusion, women have to buy the blood, which is more than 100 [US] dollars. If there is need for antibiotics, they also have to buy.”
Madziyire, the obstetrician, agrees the charges are an issue.
“Making the facilities fully equipped and stocked will encourage women to utilize them. Staff must be well motivated so that they handle patients well.”
Beatrice Zindora, a resident of Hopley, says she assists women in dire situations to deliver their babies.
Many are not registered at local clinics and hospitals, and some do not have baby supplies, such as clothes and diapers.
——————————————————————————————————————-
“We are in a situation where the public system is requesting women to bring everything needed for their care — things like pads, methylated spirit, cord clamps.”
EDINAH MASIYIWA, WOMEN’S ACTION GROUP
——————————————————————————————————————-
“I do this for free and out of my desire to help women,” Zindora says.
A few days earlier, she says, a woman came who could not walk or talk because she was in so much pain. The baby was coming legs first.
“I had to insert my hands inside the woman to bring the baby outside. The baby did not cry for a moment and I was panicking, but later he cried. After the birth of the child, I encouraged them to visit the hospital.”
A year ago, Magnus Kundanai gave birth at a church shrine because it was too late for her to go to the nearest clinic and she could not afford the transport — despite the fact that she had already paid US$25 in advance to give birth at the clinic, which took her three months to raise.
“Such an amount is hard to earn.”
Madziyire suggests that the Ministry of Health and Child Care train and certify the attendants at the shrines and also inspect and certify the independent facilities used for delivery.
(Linda Mujuru/Global Press Journal)
Clothes for Tatenda Mangwanya’s baby hang on a line at her house in Hopley, Harare, Zimbabwe
Gondongwe says the ministry is working to expand health facilities.
“It is the ministry’s desire that everyone is within a 10-kilometre radius of a health facility, and it has been working towards the achievement of this mission. However, there are some hard-to-reach communities which had not realized this target.”
But for young mothers like Mangwanya, home births are still preferable.
“After being treated well at the shrine, if the health care system does not improve, I am likely to return to Takaedza for assistance,” she says with a smile.
Unicef’s Adolescent Pregnancies in Zimbabwe report published recently by the Health and Child Care ministry and Unicef with the support of the United Nations Population Fund (UNFPA) and Unesco, indicates an adolescent pregnancy prevalence rate in Zimbabwe of 23,7%
A SIGNIFICANT chunk of the pregnancies attended to at some health institutions across the country involved adolescent girls under 19 years a United Nations Children’s Fund (Unicef) report has revealed.
Unicef’s Adolescent Pregnancies in Zimbabwe report published recently by the Health and Child Care ministry and Unicef with the support of the United Nations Population Fund (UNFPA) and Unesco, indicates an adolescent pregnancy prevalence rate in Zimbabwe of 23,7%.
The UN agency said the Health Resilience Fund being spearheaded by the government, development and technical partners is tackling such issues through efforts to improve access to primary healthcare services.
The Health Resilience Fund is a co-ordinated effort by the government and development and technical partners supporting the Health and Child Care ministry to attain universal health coverage for Zimbabweans.
It is also led by the Health and Child Care ministry and benefits from financial contributions from the European Union, the governments of Ireland and the United Kingdom, Gavi, the Vaccine Alliance and technical support from UNFPA, Unicef, and the World Health Organisation.
Its programmes are implemented at national, provincial, district and community levels by implementing partners.
According to Unicef, the fund assists Plumtree District Hospital by training healthcare workers, providing clinical mentorship for doctor-nurse teams, and providing health supplies and medicines.
Particular attention is given to the health of adolescent girls, as Zimbabwe faces high levels of early pregnancies.
“The Adolescent Pregnancies in Zimbabwe, published recently by the Ministry of Health and Child Care and Unicef with the support of UNFPA and Unesco, indicates an adolescent pregnancy prevalence rate in Zimbabwe of 23,7%.
“At Plumtree District Hospital, 29 out of the 34 mothers seen at the maternity waiting home on the visit day were adolescents under 19,” the report indicated.
Unicef also said accessing essential medicines was key to the Health Resilience Fund’s ultimate objective.
The report further indicated: “This accessibility contributes to ensuring universal health coverage for all Zimbabweans, meaning everyone in Zimbabwe has access to a full range of quality health services without financial hardship.
“Ensuring universal health coverage implies health services are brought to the people, like here through an outreach activity in Matabeleland South.
“To end preventable deaths in maternal, newborn and child health, interventions of the Health Resilience Fund emphasise increased availability, equity and access to essential reproductive maternal, newborn, child and adolescent health and nutrition services, including through promoting community participation and bringing health services as close as possible to the people’s everyday environment.”
Zimcodd said the lack of accessibility disproportionately affects pregnant women, the elderly, and the people with disability community
GOVERNMENT has been urged to heavily invest in public health because the country risks missing its United Nations Sustainable Development Goals (SDGs).
The Zimbabwe Coalition on Debt and Development (Zimcodd) made the call after a survey it conducted indicated that more than 58% of the country’s 57 districts were experiencing poor supply of essential medical drugs.
In its health and education situation report, Zimcodd said Zimbabwe’s healthcare system was plagued by inadequate finance, corruption, biased spending and lack of community involvement.
“Governments must heavily invest in public healthcare. In Africa, signatories to the Abuja Declaration of 2001, including Zimbabwe, agreed to earmark 15% of their national budgets towards public health spending,” Zimcodd said.
“Public health is critical in determining a country’s health status and economic development, as nations that spend more on healthcare will have healthier and more productive human capital, reducing health-related inequalities and powering national output [GDP] growth.”
The pressure group said 64% of the districts reported an acute shortage of healthcare personnel.
The results further indicated that 54% of the districts surveyed require increased investments in the construction of new or renovation of existing healthcare infrastructure.
It further indicated that 61% of the districts required medical equipment of the 21st century to improve public health service delivery.
Said the report: “This is in sync with official statistics showing low capital expenditure on health; for instance, only 12,5% of 2020 public spending was for health capital projects.
“More so, about 69% and 70% of the districts have poor maternal healthcare and ambulance services, respectively. It is appalling to note that the survey results show that only half of the districts have accessible healthcare facilities.”
Zimcodd argued that the results showed a deepening structural inequality — a system of privilege created by institutions within an economy.
“This lack of accessibility disproportionately affects pregnant women, the elderly, and the people with disability community,” the report said.
“However, survey results show that with a tightening economy characterised by chronic inflation and volatile local currency (Zimdollar), public sector healthcare services are affordable compared to private healthcare providers.”
It further indicated that official statistics, however, showed that the government has increased health funding from US$117 million in 2020 to an average of US$460 million from 2021 to 2024.
“The increase aligns with its commitment to the National Development Strategy 1 (NDS 1) outcome of increasing domestic funding for health.
“The NDS 1 (National Development Strategy 1) is the national policy which every other policy thrust is built upon. This is evidenced by the National Health Strategy whose objectives and pillars are in alignment with the NDS 1 health targets,” Zimcodd added.
It further indicated that to address the barriers and improve healthcare delivery there is need for increased community participation and better equipped lower-level health facilities.
It called for enhanced citizen expenditure monitoring, staff retention measures and increased resource allocation.
CONCERNS have been raised over the deteriorating state of Mpilo Hospital which is in dire straits with one malfunctioning radiotherapy machine and no accommodation for patients awaiting treatment.
Mpilo is the biggest referral hospital servicing Bulawayo and some parts of Matabeleland and according to senators is taking a strain.
Bulawayo senator, Linda Sibanda said the radiotherapy which has been malfunctioning for four years is disadvantageous to cancer patients.
“The radiotherapy machine at Mpilo Hospital has not been functional since August 2020, which is four years back. When you are doing radiation there, you are given about 23 sessions to do using a radiotherapy machine.
“I had to undergo therapy there and I think I only did 17 sessions and the machine broke down. Up to now, the machine has not been working. We have got so many people suffering from different cancers in Zimbabwe and Mpilo Hospital is one of the biggest referral hospitals. Now, it is four years since the machine broke down,” said Sibanda.
The situation at Mpilo Hospital is a reflection of the state of public healthcare institutions in the country which are buckling under maladministration and lack of proper funding.
Zimbabwe’s health sector has been under strain with hospitals understaffed and lack of medical sundries.
Lilian Mlilo concurred with Sibanda adding that patients at Mpilo Hospital are sleeping on the floor as a result of inadequate accommodation.
“My question has already been asked as part of a question, but I am going to talk about Mpilo Hospital as a referral hospital.
“Looking at the whole of Matabeleland, particularly considering the population and the huge traffic of people who go to Mpilo, what plans has the Minister in terms of assisting people so that they get accommodation instead of sleeping on the floor,” said Mlilo.
The World Health Organisation has set a target of 60% coverage of childhood cancers by the year 2030 and Zimbabwe is still lagging at 20%
Stakeholders in the healthcare sector have decried the late presentation of childhood cancer cases saying that it was a derailing efforts to fight the disease.
The World Health Organisation set a target of 60% coverage of childhood cancers by the year 2030 and Zimbabwe is still lagging at 20%.
Speaking on the sidelines of the Husqvarna Kidzcan Mud Run fundraising event on Saturday last week, cancer care nurse Charity Kawadza said they were making efforts to ensure that the survival rate of childhood cancer patients increases.
“Zimbabwe is a country which has been designated in the low to medium income countries catergory, which means our survival rate is about 20%.
“We want to raise the survival rate as high as possible. If we can get as high as 60%, which is being advocated for by World Health Organisation by the year 2030,” she said.
Kawadza said as a result of the aim to eliminate childhood cancers they had come up with a home for patients where they are given support and shelter as they undergo treatment processes.
“The other part we’ve added recently, which is a year old, is the home, what we call a halfway home. It is called Rainbow Children’s Village.
“It’s under three partners, KidzaCan, Meikles Foundation and Roundtable. Patients who come to stay with us at the village are those who are in between treatment.
“They would have already started treatment and they need a small break, but they cannot go home, which is maybe too far, so we house them until they get to their next appointment.
“We are giving drugs, giving all the support, but the element of treatment adherence is also very important. The number one cancer for children in Zimbabwe is leukemia, which is a blood cancer,” she said.
Mud Run founder Grant Mitchell said they were raising funds for KidzCan, adding that the organisation was doing a great job in the fight against childhood cancers.
“This is the 12th consecutive year. We didn’t stop through COVID. We were able to keep the event going through the years of COVID, obviously under the watchful eye of the SRC and the ministry,” Mitchell said.
The Ministry of Health and Child Care (MoHCC) has reported a total of 1,588 confirmed cases and five fatalities of malaria within a single week.
According to the Disease Surveillance Report for the week concluding on March 24, 2024, the MoHCC highlighted that among the reported cases, 140 affected children were under the age of five.
The report outlined specific locations of the fatalities, notably including Centenary district (1) and Mt Darwin district (1) within Mash Central province, district (2) in Masvingo province, and Mpilo Central Hospital in Bulawayo province.
Mashonaland Central province documented the highest number of cases at 901, followed by Manicaland province with 243 cases.
These statistics contribute to a cumulative total of 10,957 malaria cases and 15 fatalities nationwide.
Malaria, an infectious disease transmitted by mosquitoes, continues to pose a significant health threat, particularly in sub-Saharan Africa.
Given Zimbabwe’s warm and humid climate, the nation remains especially vulnerable to malaria outbreaks, particularly during the rainy season.
In other health-related news, this week witnessed the reporting of 525 cases of dog bites, with no recorded fatalities.
Among these incidents, 131 individuals were bitten by vaccinated dogs, 190 by unvaccinated dogs, and 204 by dogs with an unknown vaccination status, as outlined by the ministry in a public notice.
HEALTH and Child Care minister Douglas Mombeshora has admitted that the brain drain has left the health sector on its knees, denying patients access to primary medical attention.
Mombeshora revealed this in Parliament this week, while responding to written submissions made by legislators on the state of the health sector in the country.
He said the ministry is struggling to fill vacant posts.
“The Ministry of Health and Child Care is currently facing challenges with inadequate numbers of staff,” he said.
“This has been exacerbated by the cholera outbreak and building of new facilities which have increased the burden on the staffing levels at institutions across the country.”
“The Health Service Commission continues to engage with the Treasury, seeking creation of new posts to enable the ministry to adequately staff both the existing and new health institutions.”
The health sector has been hard-hit by a mass exodus of doctors, nurses and other experienced personnel protesting poor salaries and working conditions.
Most of the health professionals have left for the United Kingdom in recent years, with estimates putting the figure at over 3 000 since 2022.
In 2018, Vice-President Constantino Chiwenga grabbed international headlines after firing over 15 000 striking nurses.
He was forced to reverse the decision a few days later.
Chiwenga was accused of using “military-style tactics” to intimidate health workers from downing tools.
During his time, the ministry announced plans to ban doctors and nurses from striking for more than three days under proposed amendments to the Health Services Act.
Under the changes, worker representatives charged for inciting nurses and doctors to embark on strike action deemed illegal faced jail terms.




















Recent Comments