Cholera vaccine supplies are tight as Southern Africa’s outbreak crosses into SA.
Two cholera cases linked to Zimbabwe have been detected in Limpopo.
The Red Cross is looking for R88 million in funding to promote access to clean water in cholera-hit areas of Zambia.
A multi-country cholera outbreak covering Zimbabwe, Malawi and Zambia – with isolated cases now detected in South Africa – could be hard to contain thanks to a shortage of vaccine supplies.
Preliminary data indicate that the number of cholera cases reported in 2023 has exceeded that of 2022, with over 667 000 cases and 4 000 deaths globally.
According to the World Health Organisation (WHO), cholera’s resurgence in 2021 was linked to climate change issues such as flooding, coupled with poor sanitation and bad infrastructure in some countries, and was classified as a Grade 3 emergency, requiring top priority attention.
Outbreak statistics “must be interpreted with caution given the varying surveillance systems and capacity across countries, which means that 2023 data are not directly comparable to reports from previous years”, WHO said in a statement.
It has since asked its partners and governments to double their efforts in countering cholera, and that money is urgently needed to execute this mission.
“As cholera cases surge, there is a need to redouble efforts, with every citizen, organisation, and authority playing their part in turning this tide. Increased funding and unwavering collaboration are now indispensable weapons in the fight against this preventable disease. Only through a unified effort, bolstered by adequate resources, can we curb the spread of cholera,” WHO said.
THE SPREAD
In December, South Africa ramped up efforts to screen people returning from Zimbabwe, one of the countries hardest hit by the outbreak.
But cholera cases linked to Zimbabwe have since been recorded in South Africa.
In a statement this week, Limpopo health department spokesperson Thilivhali Muavha said two suspected cholera cases in the province had been detected in Zimbabweans.
“The patients, both Zimbabwean men, aged 43 and 27, who upon their return from the festivities presented to Musina and Hellen Franz Hospitals, respectively, with cholera-like symptoms,” she added.
Harare, Zimbabwe’s capital city, is the hardest hit by cholera in the country.
With the help of health partners such as WHO, in a bid to contain a spread that has become countrywide, cholera treatment centres have been decentralised.
The centres are located near affected communities so that those infected don’t have to walk long distances, which risks spreading the disease.
“By prioritising accessibility and community engagement, the decentralisation of treatment centres offers a promising solution for curbing the spread of the disease, reducing mortality, and ensuring the well-being of Zimbabweans,” said professor Jean-Marie Dangou, the WHO representative in Zimbabwe.
Zimbabwean presidential spokesperson George Charamba told journalists that “investigations by our health officials have revealed that most victims of the current wave of cholera in the Chiredzi irrigation zones helped themselves to untreated water in canals meant for irrigation. People should avoid taking such raw water; it is contaminated and thus deadly”.
The count in Zimbabwe as of Monday stood at 15 137 suspected cholera cases, 1 959 confirmed cases, 14 578 recoveries, 67 confirmed deaths, and 266 suspected deaths.
In Zambia, President Hakiande Hichilema cut short his holiday to attend to a cholera crisis that was first detected in October last year in peri-urban areas around Lusaka, putting an estimated 10 million people at risk.
There are more than 9 500 cholera cases and 374 deaths registered in Zambia, with a case fatality rate of 3.9%.
The International Federation of Red Cross and Red Crescent Societies (IFRC) has since launched an R88-million emergency appeal to address the cholera outbreak in Zambia.
The money would be channeled towards the provision of clean water.
“To ensure no more lives are lost, we must prioritise access to clean and safe water. With the waterborne disease spreading rapidly, we are deeply concerned about the situation unfolding. The IFRC and Zambia Red Cross Society are seeking resources to contribute to activities that can support stopping the spread and its transmission,” said John Roche, IFRC Head of Delegation Country Cluster for Zimbabwe, Zambia and Malawi.
Between 2022-23, Malawi faced one of its worst cholera outbreaks which led to the highest number of cholera deaths in a single country in 2023, a World Health Organisation (WHO) report shows.
As of August 2023, there were 58 982 cholera cases in Malawi, with 1 768 deaths reported. While things have subsided a bit, new cases of cholera in Malawi are linked to neighbouring countries.
On Sunday, a truck driver was admitted to Bwaila Hospital in Lilongwe due to cholera suspected to have been imported from Zambia.
Late last year in the DRC, increased conflict and displacement in the eastern part of the country pushed children into the worst cholera crisis since 2017.
The initiative, started in 2006, addresses the shortage of psychosocial help and abundance of mental health issues in Zimbabwe.
Zimbabwe’s Friendship Bench counselling service has been replicated in African countries such as Tanzania, Malawi, Kenya and Botswana [Courtesy of The Friendship Bench]
Harare, Zimbabwe – In Zimbabwe, a country of 15 million people, there are fewer than 20 psychiatrists.
And mental health issues are rife, given a litany of trauma unaddressed for decades: first the horrors of British colonialism and the liberation struggle and then the Zimbabwean army’s killing of thousands of people in the southwestern region of Matabeleland for allegedly supporting ex-guerrillas who turned on the government after independence.
Even today, the impact of socioeconomic hardships resulting from a faltering economy, high unemployment and the highest inflation rate in the world along with an ailing healthcare system have made the Southern African country fertile ground for depression, post-traumatic stress disorder, domestic violence and suicide.
According to the World Health Organization (WHO), Zimbabwe has one of the highest suicide rates in Africa.
Consequently, most people living with mental health issues, especially those who cannot afford the steep psychiatrist fees, do not get any help.
It is against this backdrop that psychiatrist Dr Dixon Chibanda came up with the idea of training lay health workers to counsel those struggling with mental health problems.
Two unrelated, tragic events prodded him into action. The first was the 2004 suicide of Erica, a patient he had been treating for three years, after she failed to raise the bus fare to travel to Harare for a follow-up session at the government hospital where he worked. The fare was less than $20.
”I was stunned, heartbroken and felt guilty when her mother called me to say she had taken her own life,” Chibanda says.
A few months later, the government razed tens of thousands of unauthorised residential properties across the country. The exercise, called Murambatsvina, or Reject the Filth, created at least 700,000 homeless people. This inevitably led to an increase in the number of people in need of mental health support.
After the much-criticized home demolitions, described by the United Nations as a violation of international law, the authorities decided there was a need for some psychological intervention.
“But there was no money or trained personnel to implement a programme. Nurses and doctors in any primary health facility are always overworked,” an exasperated Chibanda says.
A grandmother sits with a male patient during a Friendship Bench session [Ish Mafundikwa_Al Jazeera]
THE RISE OF THE GRANDMOTHERS
The only people available were elderly female community health workers at Harare City Council clinics who were unskilled for psychosocial work. So Chibanda worked with the Ministry of Health and Child Care and the University of Zimbabwe to develop a pilot programme in 2006 that trained 14 lay health workers, popularly referred to as grandmothers, in evidence-based problem-solving therapy. The grandmothers on average are 50 years of age.
“Grandmothers are rooted in communities, and they are the custodians of our culture and wisdom and already play a pivotal role in problem-solving in communities,” Chibanda says. Grandfathers have signed up as counsellors too, but he says they lack the commitment of the grandmothers. “They are unreliable and often leave because they have to get jobs or do other things.”
The training aimed to enhance the grandmothers’ listening skills, empathy and abilities to help patients gain the confidence to find solutions to their problems. It equipped them with the tools to counsel patients with common mental health disorders such as depression and anxiety. Those with more severe problems are referred to mental health professionals.
The initiative became known as The Friendship Bench because the counselling happens on made-for-purpose benches.
One of the thousands of people who have benefitted from The Friendship Bench is Blessing (not her real name), a 45-year-old mother of two who started going to the bench in 2018.
“I was down because my husband, who had relocated to South Africa to find a job, had taken another wife and had stopped sending money home,” she says. She is also HIV-positive. “I was reluctant to engage the grandmother who approached me when I went to the local clinic for treatment because I feared they would spread the word that I was on antiretrovirals.”
“But I felt better after three sessions. They pointed me in the right direction. The grannies are now my friends.”
Some of the HelpAge USA counsellors working on a similar Friendship Bench initiative [Courtesy of HelpAge USA]
HOW IT WORKS
The grandmothers make it clear to whomever they are counselling that The Friendship Bench does not give cash handouts. What they do is discuss possible solutions with their clients. ”Sometimes the solution is as easy as getting a loan from a relative or a friend, but because the client feels overwhelmed, they cannot think about those options,” says grandmother Ngabu, who counselled Blessing.
She says it usually takes three or four sessions for a client to start to see some light.
Blessing had a vending hustle going, but it was not making much money because she did not have the capital to order enough stock. That changed when 59-year-old Ngabu encouraged her to join a savings club in which women get together and save an agreed amount every week or month, and one of them gets paid out every month or week.
“My business has grown, and I make enough to send my children to school,” Blessing tells Al Jazeera. “The oldest, a 22-year-old young man, finished high school and is now a plumbing apprentice. The girl, now 18, is in her final year of high school and wants to be a lawyer.”
Her husband has stopped communicating with the family, but Blessing is not bothered, “My biggest worry was educating my children,” she says, “I am managing that, and we are happy.”
Like many others in Zimbabwe, Blessing was unaware that she was suffering from depression. “I feared I was going insane,” she says.
The Friendship Bench grandmother who approached her was trained to identify patients who came to the clinic with other ailments but also had mental health issues. The minute Blessing trusted the grandmother, she went through a process several others had gone through and are still going through.
“ I was invited to sit on a bench on the clinic grounds with grandmother Ngabu, who told me that what we discussed was confidential,” she recollects. “She then asked me a list of questions.”
The questions are on a form called the 14-point symptoms questionnaire. How patients answer determines the level of mental health problems they are experiencing. If they are suicidal or have a severe mental illness, they are referred to a more experienced grandmother, a clinical psychologist or a psychiatrist.
A six-month randomized clinical trial by local and international mental health professionals in 2014 and 2015 gave the initiative a thumbs-up. In a Journal of the American Medical Association report, they concluded: “The use of lay health workers in resource-poor countries like Zimbabwe may be effective primary care-based management of common mental disorders.”
FROM LOCAL NEED TO GLOBAL NEED
That seal of approval has seen The Friendship Bench replicated in African countries such as Tanzania, Malawi, Kenya and Botswana with Zambia and Rwanda next. A digital version of Friendship Bench is also currently used in parts of North Africa.
The Friendship Bench has also been replicated in a few resource-rich countries, dispelling the myth that it is only for poor countries. It has also turned the widespread belief that ideas and innovations migrate only from the Global North to the Global South on its head.
Chibanda is still coming to terms with how it has gone global: “The idea was to respond to a local need. Little did I know that what we were responding to was a global need.”
HelpAge USA, an international nonprofit that champions the welfare of older people in more than 80 countries, is piloting The Friendship Bench in Washington, DC, in early 2024. Cindy Cox-Roman, the organization’s chief executive, tells Al Jazeera that the intervention transcends countries. “It’s really about human connection. We have a mental health crisis in the US that manifests itself in many different ways, and it cuts across income and ethnicity. It affects everyone.”
HelpAge’s US Friendship Bench echoes the original version of the programme in Zimbabwe. It started by training 20 older people, 17 of whom are women. “This group of elderly people is interested in doing something about mental health in DC. It’s all about how people can support others struggling with difficult thoughts and feelings,” Cox-Roman says.
She says that while there may be more trained mental health professionals in the United States, more are needed. “Someone may seek professional mental health support but then have to wait for three months to see a professional.” She hopes The Friendship Bench will provide quick access to those who need help.
The volunteer counsellors in Washington, DC, are all Black and will work in their communities. “There are fewer resources in the Black community, and there is also stigma that cuts across race, ethnicity, income, etc. Part of what we want to do is tackle that stigma by normalizing mental health struggles,” Cox-Roman says.
Unlike in Zimbabwe, though, the benches in Washington will be in places such as libraries and places of worship because, according to Cox-Roman, “The safety of our older volunteers is of paramount importance to us. We don’t want to expose them to unnecessary danger.”
The one-year pilot will look at the feasibility and acceptability of the project, after which it will be evaluated and tweaked according to local needs.
During the mayorship of Bill de Blasio in New York City, it was piloted in the Bronx and Harlem with more than 60,000 people receiving therapy. The experiment petered out because of a lack of funding after de Blasio left office two years ago.
In Jamaica, Robert Dunn, a Netherlands-based psychotherapist, has, with the University of the West Indies in Kingston, carried out preliminary work to establish The Friendship Bench on the island. Jordan and Vietnam have also successfully replicated the initiative, Chibanda tells Al Jazeera.
In another vote of confidence, the WHO and Qatar got together to install 32 benches representing each of the participating countries during the 2022 World Cup. They were set up across Doha and outside tournament stadiums.
At the time, WHO Director-General Tedros Adhanom Ghebreyesus spoke highly of The Friendship Bench project: “The bench is a simple yet powerful vehicle for promoting mental health, from park benches to football stadiums.”
Chibanda says no actual counselling took place on the 32 benches. “It was not really therapy as such, just showcasing the bench and demystifying mental health,” the doctor says.
And while he welcomes replication of the bench, he says some cut corners and create their own knockoffs. Some don’t acknowledge where the idea came from.
“They take on the model and present it as something they have conceptualized. That raises questions about fidelity – how do we know they are doing the right thing?” Even worse, he says, in some places, people are being charged for the services. “ It was never my idea to charge people for sitting on the bench.”
Dr Dixon Chibanda accepts the 2023 McNulty Prize for ‘revolutionising mental healthcare by bringing therapy directly to communities via trained grandmothers’ [Courtesy of Aspen Institute/Jared Sisken]
AN EXPANDING INITIATIVE
While the plaudits of fellow mental health professionals matter, the programme’s success has also attracted the attention of philanthropists who have donated substantial sums of money to what started as a self-funded project by Chibanda.
In 2022, MacKenzie Scott, Amazon founder Jeff Bezos’s ex-wife, gave The Friendship Bench $2m. Last year, it was one of three organizations that shared the $450,000 McNulty Foundation and Aspen Institute’s John P McNulty Prize.
A Zimbabwean couple who now lives in Australia also donated a house in suburban Harare.
Chibanda is excited about the prospects for the place. “That property is worth at least around $2m. We want to convert it into a therapeutic village where the community can come for spiritual healing, practice yoga and meditate. We also intend to have a library there.”
Chibanda says others who want no publicity have also made substantial donations.
The funds have enabled The Friendship Bench to grow from an annual budget of $30,000 to $6m over the past five years.
It now employs more than 50 full-time employees and about 3,000 counsellors who have helped more than 300,000 people across Zimbabwe, and the benches are not limited to just clinics any more.
The grandmothers, who started as unpaid volunteers, now get a $25 monthly allowance, stationary and bicycles, particularly those in rural areas. Some also get a smartphone because counselling can now also be done on WhatsApp. This innovation proved popular during the COVID-19 pandemic.
The success of The Friendship Bench has also led to Chibanda becoming a respected and in-demand authority on mental health globally. The 56-year-old, Slovakia-trained doctor has spoken at international forums, including the World Economic Forum in Davos, Switzerland, and the UN General Assembly.
Besides being CEO of The Friendship Bench, he still works at a local referral hospital, runs his practice, and teaches at the University of Zimbabwe and the London School of Hygiene and Tropical Medicine.
The Friendship Bench has grown phenomenally over the past 17 years, and Chibanda has plans to make it an integral part of healthcare in Zimbabwe. He is working with the Health Ministry to do that.
“We believe that ultimately The Friendship Bench should become a government programme, so we are strengthening systems and structures within the ministry to ensure that it is integrated and becomes part and parcel of the work that government does.”
WHO staff engages nurses at Highfield Clinic in Harare
The recent surge in cholera cases has placed immense pressure on healthcare facilities, particularly the Beatrice Road Infectious Disease Hospital (BRIDH) in Harare.
To alleviate this strain and ensure accessible treatment for all, the Ministry of Health and Child Care, Harare City Council with the generous support of the World Health Organization (WHO), has started decentralising cholera treatment centers (CTC).
Two new cholera treatment centers (CTCs) are now operational, strategically located at Highfields and Budiriro polyclinics.
These facilities, with 10-bed capacities and supplies for 100 cases (40 severe, 60 moderate), bring vital medical care closer to the most affected communities.
Recommended water, sanitation and hygiene (WASH) facilities have also been installed at both centers.
“Ideally cholera cases should be managed at source and people have been coming to BRIDH where we normally manage severe cases and this has overwhelmed the facility,” said Dr Prosper Chonzi, Harare City health services director.
“This process of decentralisation of services is really key to improve quality of care,” he said.
Setting up of a CTC on a raised platform in Budiriro
By creating additional treatment centers closer to affected communities, patients suffering from cholera will no longer face long waiting times and overcrowded facilities.
This translates to quicker diagnosis, faster access to life-saving treatment, and ultimately, better patient outcomes.
In addition, decentralised centres will allow for more efficient case management, reducing the risk of further transmission within the densely populated urban areas.
Training for the health personnel manning the centers has also been done.
The new centres will also serve as hubs for health education, offering residents vital information about hygiene practices, safe water sources, and proper sanitation measures.
This empowers communities to play an active role in curbing the spread of the disease and strengthens their long-term resilience against future outbreaks.
The construction of the Highfields and Budiriro CTCs brings the total number of WHO supported centres to nine, a total of 130 beds distributed.
These treatment centres are being established or upgraded in high cholera burdened areas.
In Manicaland, two centres were upgraded at Chiadzwa and Zvipiripiri Rural Health Centres, one at Pore Pore clinic in Masvingo, and one in Harare at BRIDH.
Similarly in Harare, support has been provided to St Mary’s Polyclinic, Chitungwiza Central hospital and Stoneridge Polyclinic.
Funding for these activities is coming from the Health Resilience Fund, co-funded by the European Union, Gavi, The Vaccine Alliance and the Governments of Ireland and the United Kingdom.
WHO support extends beyond these new centers. They expanded bed capacity at Glenview Polyclinic CTC and improved patient care standards at Chitungwiza General Hospital CTC.
While BRIDH remains the city’s mainstay for infectious diseases, including cholera, the decentralisation initiative offers much-needed relief and improved access to care for affected communities.
“This initiative is a testament to the collaborative efforts of the government, healthcare providers, and international partners in tackling the cholera outbreak. By prioritising accessibility and community engagement, the decentralisation of treatment centers offers a promising solution for curbing the spread of the disease, reducing mortality and ensuring the well-being of Zimbabweans,” said professor Jean-Marie Dangou, WHO Representative to Zimbabwe.
Bilharzia, a parasitic worm that uses snails as a vector, is endemic to Zimbabwe, and could get more difficult to manage as weather patterns and temperatures shift, experts say.
With increased water shortage, people are fetching water from unprotected sources, putting their lives on danger. Credit: Derick Matsengarwodzi
THE cracking sound of whips, mingled with the din of barking dogs, yelling livestock herders, and bellowing bulls signals a new day in Marange. The village, a little over 250km from Harare, Zimbabwe’s capital, receives little rainfall, and the land is barely productive enough to comfortably sustain human lives, so livestock often go hungry.
While elders work the fields, the herding is assigned to younger boys. By 09:00, when the young herders leave for the grazing plains, the temperatures are sweltering – the vast majority of Marange’s residents say summers here have gotten hotter, and droughts have gotten more prevalent in the last ten to fifteen years.
“Children play in dirty, infected waters, some might refuse to take the medicine, and we insist on them taking the medication at the clinic. We also encounter religious sects who refuse medication.”
– Lucy Mwatamisa, nurse in Marange
Tending to livestock when pasture is scarce is a tedious task. But for Tafadzwa, aged 12, who comes from the city and visits the village on school holidays, it was an outing with friends, and a chance to plunge into the river and cool off – his parents’ warnings about the risks of swimming ignored.
Dangerous waters
Home again after the holidays, Tafadzwa began to complain of stomach pain and headaches. Soon he started passing bloody urine. His parents were worried. A visit to the clinic exposed his secret holiday escapades. “On my first visit to the clinic, they told me it was bilharzia, and it was caused by swimming in dirty water,” Tafadzwa said. “The interrogation revealed that I was playing in the river, against my parents’ warning not to do so, since it put my life at risk.”
Bilharzia, or schistosomiasis, is one of the neglected tropical diseases (NTDs) that Zimbabwe is fighting to contain, and is one of the top ten reasons for hospital admissions in the country. Freshwater snails act as a vector for the parasitic disease, which is caused by trematode flatworms that release larvae. Those larvae can penetrate the skin, so people get infected when they get into contact with the water.
Intestinal bilharzia can result in abdominal pain, diarrhoea, and blood in the stool. Urogenital bilharzia usually manifests in bloody urine, but in advanced disease, painful complications can develop.
A boy near an unprotected well in Epworth, a dormitory town in the south-eastern part of Harare. Credit: Emma Zihonye
Delays in treatment, according to Leonard Maisiri, a nurse in Kotwa, Mudzi District, can result in serious health complications. “In severe cases, bilharzia can result in bladder cancers, and in women it can affect the uterus, and [cause] pain during sexual intercourse, a condition called female genital schistosomiasis. It can also cause anaemia because of bleeding, and may result in delayed child development.”
Deaths are hard to track, because they occur via “hidden pathologies” – liver failure, bladder cancer or ectopic pregnancy, for instance – and WHO suggests that its official estimate of 11,792 mortalities a year is likely low.
Lucy Mwatamisa, a nurse in Marange, said attending to boys of Tafadzwa’s age with bilharzia symptoms has become increasingly regular. “At our clinic, we normally attend to three to five bilharzia cases of boys aged from 5 to 17 years per week, who are still in school. It is very rare to have bilharzia cases of adults or girls.”
Beating back bilharzia
In recent years, mass drug administration, such as the free treatment campaigns for 300,000 pupils in 2020, and 1.8 million children in 2022, helped to reduce the disease burden. They’ve been effective: between 2010 and 2018, Zimbabwe’s bilharzia prevalence is understood to have fallen from 23% to 5%.
“The bilharzia burden fell in 2018, as per the impact assessment carried out. It showed that there had been a decline of the burden between the first mapping in 2010 and the date of the first impact assessment in 2018 following six rounds of mass drug administration with praziquantel,” said Dr Anderson Chimusoro, Cluster Lead for Communicable and Non-Communicable Diseases at WHO Zimbabwe.
“Even though the general trend was a decline in the burden, there were a few areas which either showed no decline, as well as other areas which showed a rise in burden, particularly those which had not received mass drug administration,” revealed Dr Chimusoro.
This year, a bilharzia-control project run jointly by Zimbabwean national health bodies and China’s National Institute of Parasitic Diseases was launched in Shamva District, which has the highest prevalence of bilharzia in the country. “This is a pilot stage or study that we have conducted and launched to be able to assess the various tools that will be used for the control of the vector snails or intermediate host snails that are responsible for the transmission of bilharzia,” said Professor Nicholas Midzi, of Zimbabwe’s National Institute of Health Research (NIHR), during the launch.
To mitigate the spread of the disease, nurses Maisiri and Mwatamisa say they use the opportunity presented by routine vaccination campaigns to raise awareness of the risks of bilharzia. “When we go out for vaccination campaigns, we offer health education to young children, telling them not to play or swim in dirty water bodies, where they can get infected with bilharzia. We also encourage them not to defecate and urinate in open water sources to reduce the spread of bilharzia.”
Mwatamisa, however, said despite their efforts, health personnel still encounter some problems. “The main problem is negligence. Children play in dirty, infected waters, some might refuse to take the medicine, and we insist on them taking the medication at the clinic. We also encounter religious sects who refuse medication.”
Cloudy forecast
Climate change, resulting in altered rainfall patterns, warmer weather and increased incidence of extreme climatic events like droughts, may increase the risk of bilharzia in the country. Up to a point, warming temperatures may facilitate increased survival and reproductive rates for snails, while flooding can spell expanded habitats for the creatures. During droughts and heat waves, people congregate at fewer, and often more contaminated, water sources. WHO says one hotspot, Mt Darwin, a low-lying area, has recently recorded 50 cases per month.
But Dr Chimusoro explained that the suspected link between climate change and bilharzia rates moves in both directions. “We suspect a good linkage between bilharzia cases and climate change in the following: positively, in the reduction of bilharzia in certain areas which have become drier, and hence snails have shorter survival and humans are not in contact with infected snails. Negatively in that, former cooler areas which are not conducive for the survival of snails and the parasite getting warmer, and with sufficient water, snails and infected individuals start reporting higher infection rates.”
In Marange, on the sharp end of global climate change, nurse Mwatamisa sees how the rising heat, the reduced rainfall, and the disease are linking up. “Our area is very hot and we experience water shortages, and there is pressure on water sources, which are usually contaminated, and they get infected,” she said.
Maisiri, meanwhile, points out that the opposite disaster would be little better. “Bilharzia is a waterborne disease, and if there are floods it can cause the disease to spread, and whoever comes into contact with the water is at risk.”
A cholera patient lies on a hospital bed, in Harare, Zimbabwe, Sunday Nov. 19, 2023. A cholera outbreak in Zimbabwe is suspected of killing more than 150 people and infecting more than 8,000. The virulent bacterial disease is striking fear in many in the southern African country who live in impoverished and neglected areas where sanitation conditions are poor and local government failures have left them with no access to clean water.
HARARE, Zimbabwe — These days, Catherine Mangosho locks her 3-year-old grandson in the house for hours on end in an attempt to shield him from a deadly cholera outbreak in Zimbabwe.
The virulent bacterial disease is killing the young and the old in the southern African country, with health authorities reporting more than 150 suspected deaths and over 8,000 suspected cases since February.
Cholera has often broken out across Zimbabwe in recent years with deadly consequences and has surged and spread again over the last month, driven by the sometimes terrible sanitation conditions in poor, neglected townships and neighborhoods in the capital, Harare, and elsewhere.
Many like Mangosho, 50, fear their family might be next.
She points to a group of barefoot children playing street soccer near her house. The ball made from plastic bread wrappers frequently plunges into ponds of sewage. The children pick it out and continue their game.
“Those boys are playing with fire,” she said. “We buried a boy from this area last week. He was playing soccer in the street just like these boys one day. He fell sick overnight and died at the hospital. They said it was cholera.”
Since the start of the latest outbreak, Zimbabwe’s Health Ministry has recorded 8,087 suspected cholera cases and 1,241 laboratory confirmed cases. It said there have been 152 suspected cholera deaths and 51 laboratory confirmed deaths.
The country of 15 million people has been recording more than 500 cases a week since late October, the highest rate since February, said the International Federation of Red Cross and Red Crescent Societies. The group made an emergency appeal this month.
Cholera is a water-borne disease caused by ingesting contaminated food or water and can kill within hours if left untreated, yet it is usually easily treated by rehydrating patients if cases are caught in time.
The World Health Organization has said that cholera cases in Africa are rising exponentially amid a global surge. The African continent accounted for 21% of cases and 80% of deaths across the globe from 2014 to 2021, according to the WHO.
The outbreak in Zimbabwe is spreading from urban to rural areas and putting at risk over 10 million people, including more than 5 million children, said the Red Cross Federation. It said major causes were poor hygiene, but also a lack of awareness and religious practices that include self-proclaimed prophets ordering sect members to rely on prayer and items such as holy water rather than seek medical treatment.
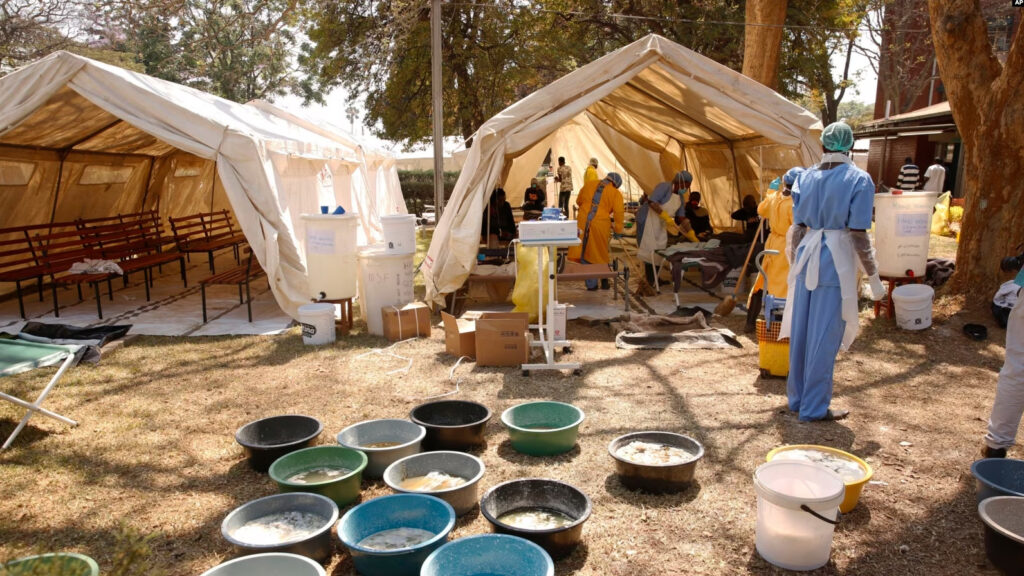
Cholera is now in all of the country’s 10 provinces, Health Minister Douglas Mombeshora said at a clinic in the hotspot township of Kuwadzana in Harare this weekend. At Kuwadzana Polyclinic, cholera patients lined up in a special tent set up for them and were given a cup of rehydrating sugar and salt solution on arrival.
“We have had a flare-up in urban areas,” said Mombeshora, adding that seven of the 13 people who have died in Harare are from Kuwadzana. “We are approaching the rainy season and the conditions cause a scare for us. We have to take it as an emergency.”
The conditions in areas like Kuwadzana and neighboring Glen View make them fertile ground for infections.
At shopping centers bustling with activity, flies crawl over heaps of uncollected trash. Raw sewage from burst pipes flows in streets and sometimes in the yards of homes. Many people have dug trenches to direct the flow away from their houses.
Long-running local government failures see many residents go for months without tap water, forcing them to dig shallow wells and boreholes that have also been contaminated by sewage.
Joyleen Nyachuru, a water, sanitation and hygiene officer with the Community Water Alliance non-governmental organization, and also a resident of the Glen View township, said she fears a repeat of 2008, when more than 4,000 people died in Zimbabwe’s worst outbreak.
“Some don’t even know the signs and symptoms of cholera, so people are just falling sick in their houses without knowing what exactly is happening to them. It’s terrifying,” said Nyachuru, who recently delivered a petition to council offices signed by dozens of residents demanding safe drinking water and an end to the dire, unhygienic conditions.
In Glen View, Mangosho is living in daily fear. She lets her grandson out for only a short while to play while watching him closely.
“The whole neighborhood has children who are sick. Some, including adults, are dying,” she said. “We are afraid.”
As Zimbabwe battles a deadly cholera outbreak in its capital Harare, patients are being treated in Kuwadzana, the epicentre of the crisis.
On Friday, authorities declared a state of emergency in Harare, a city of 1.5 million people where 13 deaths have been reported so far. Across the country, there have been 150 deaths and more than 7,000 suspected cholera cases since the outbreak began in February.
Half of the deaths in the capital have occurred in the densely-populated area of Kuwadzana, according to Zimbabwe’s health minister Dr Douglas Mombeshora.
Frequent outbreaks
Cholera outbreaks are a frequent occurrence in the country’s cities where supplies of clean water and sanitation facilities are often limited due and infrastructure has collapsed due to years of neglect.
In 2008, a cholera outbreak claimed at least 4,000 lives, with at least 100,000 cases.
More recently, in 2018, outbreaks of cholera and typhoid led the government to ramp up its vaccination efforts.
Contaminated drinking water
The disease is caused by the bacterium Vibrio cholerae which is generally transmitted through contaminated food and water.
It can be treated with an oral rehydration solution, to replace the fluids and salts lost to diarrhoea and vomiting.
President Emmerson Mnangagwa, who was re-elected in August for a second term, has promised to revitalise the country’s economy and infrastructure. In June, he pledged a nationwide borehole-drilling programme.
“We are building roads and dams and recently we started installing solar boreholes in every village across the country,” Mnangagwa said.
In highly-populated areas liked Kuwadzana, drinking water is often contaminated.
“People have dug wells close to pit latrines, especially in mushrooming settlements and other suburbs which do not have running water. This means their drinking water is contaminated,” Harare’s mayor Ian Makone said.
According to Makone, local authorities, the health ministry and aid groups have now joined forces to double the supply of water in areas affected by the current outbreak.
Masvingo, Zimbabwe – To bolster the fight against cholera and improve response activities, the Ministry of Health and Child Care (MoHCC) in collaboration with the World Health Organization (WHO) trained and equipped 54 health information officers with the necessary skills to analyze data effectively, enabling more efficient and targeted interventions. The training carried out from 13-17 November 2023, was supported by with funding from United Nations Central Emergency Response Fund (UN CERF) as well as the Contingency Fund for Emergencies (CFE).
Cholera, a highly contagious waterborne disease, continues to pose a significant public health challenge in many parts of the Zimbabwe. Rapid and accurate data analysis is crucial in understanding the spread of the disease, identifying high-risk areas, and implementing timely interventions.
MoHCC rapid diseases surveillance manager Mr Alex Goredema, emphasized the significance of this training, stating: “Accurate and timely data analysis is the backbone of effective cholera response. By investing in the training of health information officers, we are empowering them to make informed decisions that can save lives and prevent the further spread of the disease.”
The training programme covered a wide range of topics, including data collection methods, statistical analysis, data visualization, and interpretation. It incorporated both theoretical and practical components, allowing health information officers to apply their newly acquired skills to real-world scenarios. Through hands-on exercises and case studies, participants gained valuable experience in analyzing data sets specific to cholera outbreaks. This practical approach ensures that data officers are well-prepared to tackle the challenges they may encounter in the field.
Furthermore, the Ministry of Health has also established a dedicated support system to assist the health information officers (HIOs) in their work. This includes access to advanced data analysis tools and ongoing mentorship from experienced professionals. By fostering a collaborative environment, the Ministry aims to create a network of skilled health information officers who can share best practices and contribute to continuous improvement in data analysis techniques particularly during emergencies.
The impact of this training program is expected to be far-reaching. With enhanced data analysis capabilities, the Ministry of Health can identify cholera hotspots more accurately, allocate resources efficiently, and implement targeted interventions promptly. This, in turn, will help reduce the burden of cholera on affected communities and save lives.
“The training has been informative and a good refresher as we are responding to the cholera outbreak. The training provided us with the right information we need,” said Provincial Health Information Officer for Masvingo, Allen Mabhena.
Data management is one of WHO key priorities to strengthen country’s capacities for emergency preparedness to monitor the health of its population and the impact of health interventions and promote evidence-informed policy decisions. This is done through strengthening country health information, data generation, and evidence creation to address critical data gaps for priority health topics like cholera.
“Safe collection, storage, visualization and use of data are critical to planning, monitoring, and evaluation of the national health system. We are really excited that for the first time we will be incorporating predictive modeling and analysis to help identify areas were potential outbreaks may occur, giving an opportunity to adequately prepare and respond to health emergencies,” said Trevor Muchabaiwa, Data Manager at WHO Zimbabwe.
He added, “This training will ultimately ensure all policy makers have access to accurate, timely and analytical information to guarantee data driven decisions, as we continue fighting this outbreak.”
Health workers attend to patients suffering from cholera symptoms at a local hospital in Harare
Zimbabwe has declared a state of emergency in the capital Harare over a cholera outbreak.
The outbreak has so far killed dozens of people with more than 7,000 suspected cases.
The city authorities say the outbreak, spreading throughout the city, has invoked memories of a deadly outbreak in 2008, in which thousands died.
“We have declared a state of emergency because of cholera,” local media quoted Mayor Ian Makone as saying.
The authorities are now asking for help to contain the spread and provide safe water, saying the aid being received is inadequate.
Health authorities have been struggling to contain the high number of admissions following the outbreak, according to the International Federation of the Red Cross (IFRC).
It cites a lack of health workers to manage the cases, as well as lack of supplies to stop the transmission.
Zimbabwe has been battling the deadly cholera outbreak in recent months amid a lack of access to clean water.
The epicentre of the latest outbreak is Harare’s high-density suburb of Kuwadzana, which accounts for nearly half the reported cases, according to the authorities.
Cholera, an acute diarrhoeal infection is caused by consuming food or water contaminated with the bacterium Vibrio cholerae.
It is treated with an oral rehydration solution, to replace the fluids and salts lost to diarrhoea and vomiting.
On Thursday, the Harare mayor said the cholera outbreak had similarities to the 2008 outbreak.
The outbreak then led to the deaths of over 4,000 people, with at least 100,000 were infected, which led to a paralysis of basic services in the country.
This pushed then President Robert Mugabe into agreeing a historic power-sharing deal with his long-time rival, Morgan Tsvangirai.
In 2018, the country declared a state of emergency after 20 deaths and more than 2,000 cases related to typhoid and cholera were reported
“The cholera outbreak has come with vengeance,” the mayor was quoted as saying on Thursday.
On Tuesday, the ministry of health announced that the country had recorded 7,398 suspected cases, 50 confirmed deaths, and 109 people in hospital.
It came as the health minister visited the epicentre, announcing measures to deal with the outbreak – including the removal of street food vendors, and trucking of safe water.
The IFRC says the disease is quickly spreading, affecting multiple geographical areas in 45 out of 62 districts and in all 10 provinces of the country.
It says the outbreak can be expected to cross the border.
Neighbouring countries including Malawi, South Africa, and Mozambique have also frequently experienced cholera outbreaks in the past.
Cholera is now considered endemic in the Harare, which struggles with obsolete water infrastructure
Clean water shortages in townships across Zimbabwe and old, rusty water pipes could increase the severity of waterborne diseases as the rainy season, often characterised by flooding, approaches.
For Stanley Chuma, a vendor who rents a room in Cowdray Park, one of Bulawayo’s densely populated townships, the rains present a time bomb.
“In some sections, people are resorting to open wells because there’s been no water reaching us for more than two weeks.
“Imagine the dirt that you find in open sources. Rains will bring more dirty water to wells because, in some places, particularly in bushy areas, there’s open defecation,” he said.
Five litres of purified water cost about R38, he says, making it too expensive to cook with regularly. And some can’t afford to pay that much for drinking water either.
Sources from the local authority, the Bulawayo City Council (BCC), said the problem in Cowdray Park is a result of a pump failure, which was being fixed by the time of publication.
Things are worse in Harare, where some parts have gone for more than 20 years without clean running water.
Cholera is now considered endemic in the capital, which struggles with obsolete water infrastructure, a ballooning population, severe droughts, and pervasive government corruption and mismanagement.
The most recent waterborne disease outbreak comes at a time when there’s political bickering in the government and local authorities between the ruling Zanu-PF and the main opposition, the Citizens Coalition for Change (CCC).
President Emmerson Mnangagwa, writing in the state-controlled Sunday Mail, said the cholera situation was to be blamed on poorly run local authorities and the “government will not hesitate to intervene to protect lives as part of broad strategic interventions.”
He also vowed to drill 35 000 boreholes across the country before year end.
According to the Ministry of Health and Child Care’s weekly disease surveillance report released last week, cholera, typhoid, dysentery, and malaria are on the rise across the country.
For the week ending 8 October, the latest figures from the health ministry show 8 873 common diarrhoea cases and six deaths.
Of the reported cases, 3 863, or some 44%, were among children under 5 years of age.
The provinces that reported the highest number of cases were Mashonaland East Province, with 1 632, and Manicaland Province, with 1 386.
The ministry said there have been 275 385 cases and 208 deaths from common diarrhoea cumulatively.
Residents filtrate water before boiling it so that they can consume it
Zimbabwe is struggling to contain a cholera outbreak as infections pass the 5,000 mark.
Over 400 new cases were recorded over the past week.
There have been 115 deaths since February.
Government blames a lack of basic hygiene and, surprisingly, some religious groups.
This week 402 new cholera cases were recorded countrywide, with the capital, Harare, and Buhera rural district in Manicaland province being hotspots.
Zimbabwe health minister Douglas Mombeshora said, “there is any element of some religious objectors who don’t seek medical attention, who don’t really send their children to school.”
“So their knowledge is slightly less as compared to other districts; that’s why it was a bit difficult in Buhera when the epidemic erupted in Buhera district.”
“Basic hygiene that is what we are encouraging now in all provinces to scale up awareness in the communities through traditional leaders through church leaders.”
But health experts have a different explanation.
Itai Rusike from the Community Working Group on Health said, “public health fundamentals or the cause of cholera have never been properly addressed since the cholera outbreak of 2008 and 2009 which I think was a marker for the government to invest in water and sanitation infrastructure.”
“Now we are seeing cholera being reported in rural settings which is very worrying mainly because people in those rural areas are also competing for unsafe sources of water with their animals “
In a bid to curb the spread of cholera, the government has ordered that funerals, burials and other gatherings must be supervised by health officials.

























Recent Comments